

Alfred Russel Wallace: Vaccination a Delusion (S536: 1898)
Russel Wallace : Alfred Russell Wallace (sic) [[p. (1)]] VACCINATION A DELUSION Its Penal Enforcement a Crime: PROVED BY THE OFFICIAL EVIDENCE IN THE REPORTS BY  ALFRED RUSSEL WALLACE London SWAN SONNENSCHEIN & CO., LIMD. 1898 [[p. (2)]] Butler & Tanner, [[p. 3]] PREFACE This Essay has been written for the purpose of influencing Parliament, and securing the speedy abolition of the unjust, cruel, and pernicious Vaccination laws. For this purpose it has been necessary to speak plainly of the ignorance and incompetence displayed by the Royal Commission, proofs of which I give from their “Final Report” and the evidence they have collected and printed. I most solemnly urge upon our Legislators that this is a question not only of the liberties of Englishmen, but one affecting the lives of their children, and the health of the whole community; and that they will be individually responsible if they do not inquire into this matter for themselves,–not accept the statements or opinions of others. In order that they may do this with a minimum expenditure of time and labour, I have put before them the essential facts, in almost every case taken from the Reports of the Royal Commission or of the Registrar-General, and with references to page, question, or paragraph, so that they can themselves verify every statement I make. I thus abundantly prove, first, that in all previous legislation they have been misled by facts and figures that are untrue and by promises that have been all unfulfilled; and that similar misstatements have characterised the whole official advocacy of Vaccination from the time of Jenner down to this day. I claim, therefore, that all official statements as to Vaccination are untrustworthy. [[p. 4]] I then show that all the statistics of small-pox mortality, whether of London; of England, Scotland, and Ireland; of the best vaccinated Continental States; of unvaccinated Leicester; or of the revaccinated Army and Navy, without any exception, prove the absolute inutility of Vaccination; and I feel confident that every unprejudiced person who will carefully read these few pages, and will verify such of my statements as seem to them most incredible, will be compelled to come to the same conclusion. I appeal from the medical and official apologists of Vaccination to the intelligence and common sense of my fellow-countrymen, and I urge them to insist upon the immediate abolition of all legislation enforcing or supporting this useless and dangerous operation. CONTENTS Chapter I. Vaccination and Small-Pox . . . . . page 5 Chapter II. Much of the Evidence adduced for Vaccination is Worthless . . . . . 23 Chapter III. The General Statistics of Small-pox Mortality in relation to Vaccination . . . . . 31 Chapter IV. Two Great Experiments which are conclusive against Vaccination . . . . . 54 Chapter V. Critical Remarks on the “Final Report” . . . . . 70 Chapter VI. Summary and Conclusion . . . . . 80 [[p. 5]] CHAPTER I VACCINATION AND SMALL-POX Among the greatest self-created scourges of civilized humanity are the group of zymotic diseases, or those which arise from infection, and are believed to be due to the agency of minute organisms which rapidly increase in bodies offering favourable conditions, and often cause death. Such diseases are: plague, small-pox, measles, whooping-cough, yellow fever, typhus and enteric fevers, scarlet fever and diphtheria, and cholera. The conditions which especially favour these diseases are foul air and water, decaying organic matter, overcrowding, and other unwholesome surroundings, whence they have been termed “filth diseases.” The most terrible and fatal of these–the plague–prevails only where people live under the very worst sanitary conditions as regards ventilation, water supply, and general cleanliness. Till about 250 years ago it was as common in England as small-pox has been during the present century, but a very partial and limited advance in healthy conditions of life entirely abolished it, its place being to some extent taken by small-pox, cholera, and fevers. The exact mode by which all these diseases spread is not known; cholera, typhus, and enteric fever are believed to be communicated through the dejecta from the patient contaminating drinking water. The other diseases are spread either by bodily contact or by transmission of germs through [[p. 6]] the air; but with all of them there must be conditions favouring their reception and increase. Not only are many persons apparently insusceptible through life to some of these diseases, but all the evidence goes to show that, if the whole population of a country lived under thoroughly healthy conditions as regards pure air, pure water, and wholesome food, none of them could ever obtain a footing, and they would die out as completely as the plague and leprosy have died out, though both were once so prevalent in England. But during the last century there was no such knowledge, and no general belief in the efficacy of simple, healthy conditions of life as the only effectual safeguard against these diseases. Small-pox, although then, as now, an epidemic disease and of very varying degrees of virulence, was much dreaded, because, owing chiefly to improper treatment, it was often fatal, and still more often produced disfigurement or even blindness. When, therefore, the method of inoculation was introduced from the East in the early part of the eighteenth century, it was quickly welcomed, because a mild form of the disease was produced which rarely caused death or disfigurement, though it was believed to be an effectual protection against taking the disease by ordinary infection. It was, however, soon found that the mild small-pox usually produced by inoculation was quite as infectious as the natural disease, and became quite as fatal to persons who caught it. Towards the end of the last century many medical men became so impressed with its danger that they advocated more attention to sanitation and the isolation of patients, because inoculation, though it may have saved individuals, really increased the total deaths from small-pox. Under these circumstances we can well understand the favourable reception given to an operation which produced a slight, non-infectious disease, which yet was alleged to protect against small-pox as completely as did the inoculated disease itself. This was Vaccination, which arose from the belief of farmers in [[p. 7]] Gloucestershire and elsewhere that those who had caught cow-pox from cows were free from small-pox for the rest of their lives. Jenner, in 1798, published his Inquiry, giving an account of the facts which, in his opinion, proved this to be the case. But in the light of our present knowledge we see that they are wholly inconclusive. Six of his patients had had cow-pox when young, and were inoculated with small-pox in the usual way from twenty-one to fifty-three years afterwards, and because they did not take the disease, he concluded that the cow-pox had preserved them. But we know that a considerable proportion of persons in middle age are insusceptible to small-pox infection; besides which even those who most strongly uphold vaccination now admit that its effects die out entirely in a few years–some say four or five, some ten–so that these people who had had cow-pox so long before were certainly not protected by it from taking small-pox. Several other patients were farriers or stable men who were infected by horse-grease, not by cow-pox, and were also said to be insusceptible to small-pox inoculation, though not so completely as those who had had cow-pox. The remainder of Jenner’s cases were six children, from five to eight years old, who were vaccinated, and then inoculated a few weeks or months afterwards. These cases are fallacious from two causes. In the first place, any remnant of the effects of the vaccination (which were sometimes severe), or the existence of scurvy, then very prevalent, or of any other skin-disease, might prevent the test-inoculation from producing any effect.1 The other [[p. 8]] cause of uncertainty arises from the fact that this “variolous test” consisted in inoculating with small-pox virus obtained from the last of a series of successive patients in whom the effect produced was a minimum, consisting of very few pustules, sometimes only one, and a very slight amount of fever. The results of this test, whether on a person who had had cow-pox or who had not had it, was usually so slight that it could easily be described by a believer in the influence of the one disease on the other as having “no effect”; and Dr. Creighton declares, after a study of the whole literature of the subject, that the description of the results of the test is almost always loose and general, and that in the few cases where more detail is given the symptoms described are almost the same in the vaccinated as in the unvaccinated. Again, no careful tests were ever made by inoculating at the same time, and in exactly the same way, two groups of persons of similar age, constitution, and health, the one group having been vaccinated the other not, and none of them having had small-pox, and then having the resulting effects carefully described and compared by independent experts. Such “control” experiments would now be required in any case of such importance as this; but it was never done in the early days of vaccination, and it appears never to have been done to this day. The alleged “test” was, it is true, applied in a great number of cases by the early observers, especially by Dr. Woodville, physician to a small-pox hospital; but Dr. Creighton shows reason for believing that the lymph he used was contaminated with small- [[p. 9]] pox, and that the supposed vaccinations were really inoculations. This lymph was widely spread all over the country, and was supplied to Jenner himself, and we thus have explained the effect of the “vaccination” in preventing the subsequent “inoculation” from producing much effect, since both were really mild forms of small-pox inoculation. This matter is fully explained by Dr. Creighton in his evidence before the Royal Commission, printed in the Second Report. Professor E. M. Crookshank, who has made a special study of cow-pox and other animal diseases and their relation to human small-pox, gives important confirmatory evidence, to be found in the Fourth Report. This brief statement of the early history of vaccination has been introduced here in order to give what seems to be a probable explanation of the remarkable fact that a large portion of the medical profession accepted, as proved, that vaccination protected against a subsequent inoculation of small-pox, when in reality there was no such proof, as the subsequent history of small-pox epidemics has shown. The medical and other members of the Royal Commission could not realize the possibility of such a failure to get at the truth. Again and again they asked the witnesses above referred to to explain how it was possible that so many educated specialists could be thus deceived. They overlooked the fact that a century ago was, as regards the majority of the medical profession, a pre-scientific age; and nothing proves this more clearly than the absence of any systematic “control” experiments, and the extreme haste with which some of the heads of the profession expressed their belief in the lifelong protection against small-pox afforded by vaccination, only four years after the discovery had been first announced. This testimony caused Parliament to vote Jenner £10,000 in 1802. Ample proof now exists of the fallacy of this belief, since vaccination gives no protection whatever, as will be shown later on. But there was also no lack of [[p. 10]] proof of this failure to protect in the first ten years of the century; and had it not been for the unscientific haste of the medical witnesses to declare that vaccination protected against small-pox during a whole lifetime–a fact of which they had not and could not possibly have any evidence–this proof of failure would have convinced them and have prevented what is really one of the scandals of the nineteenth century. These early proofs of failure will be now briefly indicated. Only six years after the announcement of vaccination, in 1804, Dr. B. Moseley, Physician to Chelsea Hospital, published a small book on the cow-pox, containing many cases of persons who had been properly vaccinated and had afterwards had small-pox; and other cases of severe illness, injury, and even death resulting from vaccination; and these failures were admitted by the Royal Jennerian Society in their Report in 1806. Dr. William Rowley, Physician to the St. Marylebone Infirmary, in a work on Cow-pox Inoculation in 1805, which reached a third edition in 1806, gave particulars of 504 cases of small-pox and injury after vaccination, with seventy-five deaths. He says to his brother medical men: “Come and see. I have lately had some of the worst species of malignant small-pox in the Marylebone Infirmary, which many of the faculty have examined and know to have been vaccinated.” For two days he had an exhibition in his Lecture Room of a number of children suffering from terrible eruptions and other diseases after vaccination. Dr. Squirrel, formerly Resident Apothecary to the Small-pox and Inoculation Hospital, also published in 1805 numerous cases of small-pox, injuries, and death after vaccination. John Birch, a London surgeon, at first adopted vaccination and corresponded with Jenner, but soon, finding that it did not protect from small-pox and that it also produced serious and sometimes fatal diseases, he became one of its strongest opponents, and [[p. 11]]published many letters and pamphlets against it up to the time of his death in 1815. Mr. William Goldson, a surgeon at Portsea, published a pamphlet in 1804, giving many cases in his own experience of small-pox following vaccination. What made his testimony more important was that he was a believer in vaccination, and sent accounts of some of his cases to Jenner so early as 1802, but no notice was taken of them.2 Mr. Thomas Brown, a surgeon of Musselburgh, published in 1809 a volume giving his experiences of the results of vaccination. He had at first accepted and practised it. He also applied the “variolous test” with apparent success, and thereafter went on vaccinating in full confidence that it was protective against small-pox, till 1808, when, during an epidemic, many of his patients caught the disease from two to eight years after vaccination. He gives the details of forty-eight cases, all within his own personal knowledge, and he says he knew of many others. He then again tried the “variolous test,” and found twelve cases in which it entirely failed, the result being exactly as with those who were inoculated without previous vaccination. These cases, with extracts from Brown’s work, were brought before the Royal Commission by Professor Crookshank. (See 4th Report, Q. 11,852.) Again, Mr. William Tebb brought before the Commission a paper by Dr. Maclean, in the Medical Observer of 1810, giving 535 cases of small-pox after vaccination, of which 97 were fatal. He also gave 150 cases of diseases from cow-pox, with the names of ten medical men, including two Professors of Anatomy, who had suffered in their own families from vaccination. The following striking passage is quoted:–“Doctrine.–Vaccination or Cow-pox inoculation is a perfect preventive of small-pox during life. (Jenner, etc.) Refutation.–535 cases of small-pox after cow- [[p. 12]] pox. Doctrine.–Cow-pox renders small-pox milder. It is never fatal. Refutation.–97 deaths from small-pox after cow-pox and from cow-pox diseases.” The cases here referred to, of failure of vaccination to protect even for a few years, are probably only a small fraction of those that occurred, since only in exceptional cases would a doctor be able to keep his patients in view, and only one doctor here and there would publish his observations. The controversy was carried on with unusual virulence, hence perhaps the reason why the public paid so little attention to it. But unfortunately both the heads of the medical profession and the legislature had committed themselves by recognising the full claims of Jenner at too early a date and in a manner that admitted of no recall. In 1802, as already stated, the House of Commons, on the Report of its Committee, and the evidence of the leading physicians and surgeons of London–a large number of whom declared their belief that cow-pox was a perfect security against small-pox–voted Jenner £10,000. When therefore the flood of evidence poured in, showing that it did not protect, it was already too late to remedy the mischief that had been done, since the profession would not so soon acknowledge its mistake, nor would the legislature admit having hastily voted away the public money without adequate reason. The vaccinators went on vaccinating, the House of Commons gave Jenner £20,000 more in 1807, endowed vaccination with £3,000 a year in 1808, and after providing for free vaccination in 1840, made the operation compulsory in 1855, and enforced it by penalties in 1867. VACCINATION AND THE MEDICAL PROFESSION Before proceeding to adduce the conclusive evidence that now exists of the failure of vaccination, a few preliminary misconceptions must be dealt with. One of these is, that as vaccination is a surgical operation to guard against a special disease, medical men can alone judge of its value. But the fact is the very [[p. 13]] reverse, for several reasons. In the first place, they are interested parties, not merely in a pecuniary sense, but as affecting the prestige of the whole profession. In no other case should we allow interested persons to decide an important matter. Whether iron ships are safer than wooden ones is not decided by ironmasters or by shipbuilders, but by the experience of sailors and by the statistics of loss. In the administration of medicine or any other remedy for a disease, the conditions are different. The doctor applies the remedy and watches the result, and if he has a large practice he thereby obtains knowledge and experience which no other persons possess. But in the case of vaccination, and especially in the case of public vaccinators, the doctor does not see the result except by accident. Those who get small-pox go to the hospitals, or are treated by other medical men, or may have left the district, and the relation between the vaccination and the attack of small-pox can only be discovered by the accurate registration of all the cases and deaths, with the facts as to vaccination or revaccination. When these facts are accurately registered, to determine what they teach is not the business of a doctor but of a statistician, and there is much evidence to show that doctors are bad statisticians, and have a special faculty for misstating figures. This allegation is so grave and so fundamental to the question at issue, that a few facts must be given in support of it. The National Vaccine Establishment, supported by Government grants, issued periodical Reports, which were printed by order of the House of Commons, and in successive years we find the following statements: In 1812, and again in 1818, it is stated that “previous to the discovery of vaccination the average number of deaths by small-pox within the (London) Bills of Mortality was 2,000 annually; whereas in the last year only 751 persons have died of the disease, although the increase of population within the last ten years has been 133,139.” The number 2,000 is about the average small-pox [[p. 14]] deaths of the whole eighteenth century, but those of the last two decades before the publication of Jenner’s Inquiry, were 1,751 and 1,786, showing a decided fall. This, however, may pass. But when we come to the Report for 1826 we find the following: “But when we reflect that before the introduction of vaccination the average number of deaths from small-pox within the Bills of Mortality was annually about 4,000, no stronger argument can reasonably be demanded in favour of the value of this important discovery.” This monstrous figure was repeated in 1834, apparently quite forgetting the correct figure for the whole century given in 1818, and also the fact that the small-pox deaths recorded in the London Bills of Mortality in any year of the century never reached 4,000. But worse is to come; for in 1836 we have the following statement: “The annual loss of life by small-pox in the Metropolis, and within the Bills of Mortality only, before vaccination was established, exceeded 5,000, whereas in the course of last year only 300 died of the distemper.” And in the Report for 1838 this gross error is repeated; while in the next year (1839) the conclusion is drawn “that 4,000 lives are saved every year in London since vaccination so largely superseded variolation.”3 The Board of the National Vaccine Establishment consisted of the President and four Censors of the Royal College of Physicians, and the Master and two senior Wardens of the College of Surgeons. We cannot possibly suppose that they knew or believed that they were publishing untruths and grossly deceiving the public. We must, therefore, fall back upon the supposition that they were careless to such an extent [[p. 15]] as not to find out that they were authorizing successive statements of the same quantity as inconsistent with each other as 2,000 and 5,000. The next example is given by Dr. Lettsom, who, in his evidence before the Parliamentary Committee in 1802, calculated the small-pox deaths of Great Britain and Ireland before vaccination at 36,000 annually; by taking 3,000 as the annual mortality in London and multiplying by twelve, because the population was estimated to be twelve times as large. He first takes a number which is much too high, and then assumes that the mortality in the town, village, and country populations was the same as in overcrowded, filthy London! Small-pox was always present in London, while Sir Gilbert Blane tells us that in many parts of the country it was quite unknown for periods of twenty, thirty, or forty years. In 1782 Mr. Connah, a surgeon at Seaford, in Sussex, only knew of one small-pox death in eleven years among a population of 700. Cross, the historian of the Norwich epidemic in 1819, states that previous to 1805 small-pox was little known in this city of 40,000 inhabitants, and was for a time almost extinct; and yet this gross error of computing the small-pox mortality of the whole country from that of London (and computing it from wrong data) was not only accepted at the time, but has been repeated again and again down to the present day as an ascertained fact! In a speech in Parliament in defence of vaccination, Sir Lyon Playfair gave 4,000 per million as the average London death-rate by small-pox before vaccination–a number nearly double that of the last twenty years of the century, which alone affords a fair comparison. But far more amazing is the statement by the late Dr. W. B. Carpenter, in a letter to the Spectator of April, 1881, that “a hundred years ago the small-pox mortality of London alone, with its then population of under a million, was often greater in a six months’ epidemic than that of the twenty millions of England and Wales now is in any whole [[p. 16]] year.” The facts, well known to every enquirer, are: that the very highest small-pox mortality in the last century in a year was 3,992 in 1772, while in 1871 it was 7,912 in London, or more than double; and in the same year, in England and Wales, it was 23,000. This amazing and almost incredible misstatement was pointed out and acknowledged privately, but never withdrawn publicly! The late Mr. Ernest Hart, a medical man, editor of the British Medical Journal, and a great authority on sanitation, in his work entitled The Truth about Vaccination, surpasses even Dr. Carpenter in the monstrosity of his errors. At page 35 of the first edition (1880), he states that in the forty years 1728-57 and 1771-80, the average annual small-pox mortality of London was about 18,000 per million living. The actual average mortality, from the tables given in the Second Report of the Royal Commission, page 290, was a little over 2,000, the worst periods having been chosen; and taking the lowest estimates of the population at the time, the mortality per million would have been under 3,000. This great authority, therefore, has multiplied the real number by six! In a later edition this statement is omitted, but in the first edition it was no mere misprint, for it was triumphantly dwelt upon over a whole page and compared with modern rates of mortality. Yet one more official misstatement. About the year 1884 the National Health Society, with the approval of the Local Government Board, issued a tract entitled Facts concerning Vaccination for Heads of Families, in which appeared the statement, “Before the introduction of vaccination, small-pox killed 40,000 persons yearly in this country.” We have already shown that Dr. Lettsom’s figure, 36,000, was utterly unfounded, and probably three or four times greater than the truth. Here we have a semi-official and widely-distributed statement even more remote from the truth. In later issues of the same tract this particular statement is withdrawn, and a different but equally [[p. 17]]erroneous one substituted. Thus: “Before its discovery (vaccination) the mortality from small-pox in London was forty times greater than it is now.” This is an altogether vague and misleading statement. If it means that in some years of the last century it was forty times greater than in some years of this century, it is misleading, because even within the last thirty years some years have a mortality not only forty but eighty and even 200 times as great as others. (In 1875 there were ten deaths per million, while in 1871 there were 2,420 deaths per million.) If it means on an average of say twenty years, it is false. For the twenty years 1869-98 the mortality was about 300 per million, while for the last twenty years before the discovery of small-pox it was about 2,000 per million, or less than seven times as much instead of forty times! This same tract is full of other equally gross misstatements. It tells us, in large, black type, “With due care in the performance of the operation, no risk of any injurious effects from it need be feared.” The Registrar-General himself shows us that this is false in his Report for 1895, Table 17, p. lii.: Cowpox and Other Effects of Vaccination An average of 52 children officially murdered every year, and officially acknowledged, is termed “alleged injury,” which need not be feared! And these cruel falsehoods are spread broadcast over the country, and the tract bears upon its title-page–[Revised by the Local Government Board, and issued with their sanction]. [[p. 18]] As the tract bears no date, I cannot tell whether it is still issued; but it was in circulation up to the time when the Commission was sitting, and it is simply disgraceful that a Government Department should ever have given its official sanction to such a tissue of misrepresentations and palpable false statements. For these 785 deaths in fifteen years, and 390 in the preceding twenty-two years (classed as from erysipelas after vaccination), no one has been punished, and no compensation or even official apology has been given to the thousand sorrowing families. And we may be sure that these acknowledged deaths are only a small portion of what have really occurred, since the numbers have increased considerably in. the later period, during which more attention has been given to such deaths and more inquests held. It is certain that for every such death acknowledged by the medical man concerned, many are concealed under the easy method of stating some of the later symptoms as the cause of death. Thus, Mr. Henry May, Medical Officer of Health, candidly states as follows: “In certificates given by us voluntarily, and to which the public have access, it is scarcely to be expected that a medical man will give opinions which may tell against or reflect upon himself in any way. In such cases he will most likely tell the truth, but not the whole truth, and assign some prominent symptom of the disease as the cause of death. As instances of cases which may tell against the medical man himself, I will mention erysipelas from vaccination, and puerperal fever. A death from the first cause occurred not long ago in my practice; and although I had not vaccinated the child, yet, in my desire to preserve vaccination from reproach, I omitted all mention of it from my certificate of death.” (See Birmingham Medical Review, Vol III., pp. 34, 35.) That such suppressio veri is no new thing, but has been going on during the whole period of vaccination, is rendered probable by a statement in the Medical Observer of 1810, by Dr. Maclean. He says: “Very few deaths from cowpox appear in the Bills of Mortality, owing [[p. 19]] to the means which have been used to suppress a knowledge of them. Neither were deaths, diseases, and failures transmitted in great abundance from the country, not because they did not happen, but because some practitioners were interested in not seeing them, and others who did see them were afraid of announcing what they knew.” As an example of the number of cases occurring all over the country, Mr. Charles Fox, a medical man residing at Cardiff has published fifty-six cases of illness following vaccination, of which seventeen resulted in death. In only two of these, where he himself gave the certificate, was vaccination mentioned. All of these cases were examined by himself personally. Among those who survived, several were permanently injured in health, and some were crippled for life; while in most of the cases the inflammation and eruptions are so painful, and the sufferings of the children so great and so prolonged, that the mother endures continuous mental torture, lasting for weeks, months, or even years. And if one medical man can record such a mass of injury and disease in which vaccination was the palpable starting-point and certainly a contributory cause, what must be the total mass of unrecorded suffering throughout the whole country? Considering this and other evidence, together with the admitted and very natural concealment by the doctors concerned, “to save vaccination from reproach,” the estimate of Mr. Alfred Milnes, a statistician who has paid special attention to the subject, that the officially admitted deaths must be at least multiplied by twelve to obtain the real deaths from vaccination, we shall arrive at the terrible number of over 600 children and adults killed annually by this compulsory operation; while judging from the proportion of permanent injury (twenty-eight) in Mr. Fox’s fifty-six cases and seventeen deaths, about 1,000 persons annually must suffer from it throughout their lives! As confirmatory of even this large amount, the testimony of Mr. Davidson, Medical Officer of Health for Congleton, and [[p. 20]] formerly a Public Vaccinator, is important. He began an inquiry into the alleged injurious effects of vaccination, without believing that they were serious. The outcome of his investigation was startling to him. In his Annual Report for 1893, he says: “In the investigation of a single vaccination period, the fact was revealed that in quite fifty per cent. of all vaccinated in that period (about seventy), the results were abnormal, and, in a large number of these very grave injuries had been inflicted. That the results of the practice are the same elsewhere as in Congleton I have no reason to doubt, for judging from what I have seen of his method of vaccinating, our Public Vaccinator is as careful as it seems possible for a Public Vaccinator to be.” This evidence of Mr. Davidson is especially important, because it reveals the fact that, as I stated some pages back, neither Public Vaccinators nor ordinary medical men usually know anything of the injurious effects of vaccination, except in such individual cases as may occur in their practice, while all around them there may be a mass of evil results which, when systematically investigated, proves as unexpected as it is startling in its amount. This brief exposition of medical and official misstatements of facts and figures, always in favour of vaccination, might have been largely increased, but it is already sufficient to demonstrate the position I take, which is, that in this matter of Official and Compulsory Vaccination, both doctors and Government officials, however highly placed, however eminent, however honourable, are yet utterly untrustworthy. Beginning in the early years of the century, and continuing to our own times, we find the most gross and palpable blunders in figures–but always on the side of vaccination–and, on the testimony of medical men themselves, a more or less continuous perversion of the official records of vaccinal injury “in order to save vaccination from reproach.” Let this always be remembered in any discussion of the question. The facts and figures [[p. 21]] of the medical profession, and of Government officials, in regard to the question of vaccination, must never be accepted without verification. And when we consider that these misstatements, and concealments, and denials of injury, have been going on throughout the whole of the century; that penal legislation has been founded on them; that homes of the poor have been broken up; that thousands have been harried by police and magistrates, have been imprisoned and treated in every way as felons; and that, at the rate now officially admitted, a thousand children have been certainly killed by vaccination during the last twenty years, and an unknown but probably much larger number injured for life, we are driven to the conclusion that those responsible for these reckless misstatements and their terrible results have, thoughtlessly and ignorantly but none the less certainly, been guilty of a crime against liberty, against health, and against humanity, which will, before many years have passed, be universally held to be one of the foulest blots on the civilization of the nineteenth century.4 [[p. 23]] CHAPTER II MUCH OF THE EVIDENCE ADDUCED FOR VACCINATION IS WORTHLESS We will now proceed to discuss the alleged value of vaccination by means of the best and widest statistical evidence at our command; and in doing so we shall be able to show that the medical experts, who have been trusted by the Government and by the general public, are no less deficient in their power of drawing accurate conclusions from the official statistics of vaccination and small-pox mortality than they have been shown to be in their capacity for recording facts and quoting figures with precision and correctness. In the elaborate paper by Sir John Simon, on the History and Practice of Vaccination, presented to Parliament in 1857 and reprinted in the First Report of the Royal Commission, he tells us that the earlier evidence of the value of vaccination was founded on individual cases, but that now “from individual cases the appeal is to masses of national experience.” And the marginal reference is, “Evidence on the protectiveness of vaccination must now be statistical.” If this was true in 1857, how much more must it be so now, when we have forty years more of “national experience” to go upon. Dr. Guy, M.D., F.R.S., enforces this view in his paper published by the Royal Statistical Society in 1882. He says: “Is vaccination a preventive of small-pox? To this question there is, there can be, no answer except such as [[p. 24]] is couched in the language of figures.” But the language of figures, otherwise the science of statistics, is not one which he who runs may read. It is full of pitfalls for the unwary, and requires either special aptitude or special training to avoid these pitfalls and deduce from the mass of figures at our command what they really teach. A commission or committee of enquiry into this momentous question should have consisted wholly, or almost wholly, of statisticians, who would hear medical as well as official and independent evidence, would have all existing official statistics at their command, and would be able to tell us, with some show of authority, exactly what the figures proved, and what they only rendered probable on one side and on the other. But instead of such a body of experts, the Royal Commission, which for more than six years was occupied in hearing evidence and cross-examining witnesses, consisted wholly of medical men, lawyers, politicians, and country gentlemen, none of whom were trained statisticians, while the majority came to the enquiry more or less prejudiced in favour of vaccination. The report of such a body can have but little value, and I hope to satisfy my readers that it (the Majority Report) is not in accordance with the facts; that the reporters have lost themselves in the mazes of unimportant details; and that they have fallen into some of the pitfalls which encumber the path of those who, without adequate knowledge or training, attempt to deal with great masses of figures. But before proceeding to discuss the statistical evidence set forth in the reports of the Commission, I have again the disagreeable task of showing that a very large portion of it, on which the Commissioners mainly rely to justify their conclusions, is altogether untrustworthy, and must therefore be rejected whenever it is opposed to the results of the great body of more accurate statistical evidence. I allude of course to the question of the comparative small-pox mortality of the VACCINATED and the UNVACCINATED. The first [[p. 25]] point to be noticed is, that existing official evidence of the greatest value has never been made use of for the purposes of registration, and is not now available. For the last sixteen years the Registrar-General gives the deaths from small-pox under three headings. Thus, in the year 1881 he gives for London (Annual Summary, p. xxiv.): Small-pox. Vaccinated . . . . . 524 deaths. And in the year 1893, for England and Wales, the figures are (Annual Report, p. xi.): Small-pox. Vaccinated . . . . . 150 deaths. Now such figures as these, even if those under the first two headings were correct, are a perfect farce, and are totally useless for any statistical purpose. Yet every vaccination is officially recorded–since 1873 private as well as public vaccinations–and it would not have been difficult to trace almost every small-pox patient to his place of birth and get the official record of his vaccination if it exists. As the medical advisers of the Government have not done this, and give us instead partial and local statistics, usually under no official sanction and often demonstrably incorrect, every rule of evidence and every dictate of common sense entitle us to reject the fragmentary and unverified statements which they put before us. Of the frequent untrustworthiness of such statements it is necessary to give a few examples. In Notes on the Small-pox Epidemic at Birkenhead, 1877 (p. 9), Dr. F. Vacher says: “Those entered as not vaccinated were admittedly unvaccinated, or without the faintest mark. The mere assertions of patients or their friends that they were vaccinated counted for nothing.” Another medical official justifies this method of making statistics as follows: “I have always classed those as ‘unvaccinated,’ when no scar, presumably arising from [[p. 26]] vaccination, could be discovered. Individuals are constantly seen who state that they have been vaccinated, but upon whom no cicatrices can be traced. In a prognostic and a statistic point of view, it is better, and, I think, necessary, to class them as unvaccinated” (Dr. Gayton’s Report for the Homerton Hospital for 1871-2-3). The result of this method, which is certainly very general though not universal, is such a falsification of the real facts as to render them worthless for statistical purposes. It is stated by so high an authority as Sir James Paget, in his lectures on Surgical Pathology, that “cicatrices may in time wear out”; while the Vaccination Committee of the Epidemiological Society, in its Report for 1885-6, admitted that “not every cicatrice will permanently exist.” Even more important is the fact that in confluent small-pox the cicatrices are hidden, and large numbers of admissions to the hospitals are in the later stages of the disease. Dr. Russell, in his Glasgow Report (1871-2, p. 25), observes, “Sometimes persons were said to be vaccinated, but no marks could be seen, very frequently because of the abundance of the eruption. In some of those cases which recovered, an inspection before dismission discovered vaccine marks sometimes very good.” In many cases private enquiry has detected errors of this kind. In the Second Report of the Commission, pp. 219-20, a witness declared that out of six persons who died of small-pox and were reported by the medical officer of the Union to have been unvaccinated, five were found to have been vaccinated, one being a child who had been vaccinated by the very person who made the report, and another a man who had been twice revaccinated in the militia (Q. 6730-42). One other case may be given. In October, 1883, three unvaccinated children were stated in the Registrar-General’s weekly return of deaths in London to have died of small-pox, “being one, four, and nine years of age, and all from 3, Medland Street, Stepney.” On enquiry at the [[p. 27]] address given (apparently by oversight in this one case) the mother stated that the three children were hers, and that “all had been beautifully vaccinated.” This case was investigated by Mr. J. Graham Spencer, of 33, Rigault Road, Fulham Park Gardens, and the facts were published in the local papers and also in The Vaccination Inquirer of December, 1883. Several other cases were detected at Sheffield, and were adduced by Mr. A. Wheeler in his evidence before the Commission (6th Report, p. 70); and many others are to be found throughout the Anti-Vaccination periodicals. But the difficulty of tracing such misstatements is very great, as the authorities almost always refuse to give information as to the cases referred to when particular deaths from small-pox are recorded as “unvaccinated.” Why this effort at secrecy in such a matter if there is nothing to hide? Surely it is to the public interest that official statistics should be made as correct as possible; and private persons who go to much trouble and expense in order to correct errors should be welcomed as public benefactors and assisted in every way, not treated as impertinent intruders on official privacy, as is too frequently the case. The result of this prejudiced and unscientific method of registering small-pox mortality is the belief of the majority of the medical writers on the subject that there is an enormous difference between the mortality of the vaccinated and the unvaccinated, and that the difference is due to the fact of vaccination or the absence of it. The following are a few of the figures as to this point given in the Reports of the Royal Commission: Authority. . . . . . Death Rate of Vaccinated. . . . . . Death Rate of Unvaccinated. Now an immense body of statistics of the last century [[p. 28]] compiled by disinterested persons who had no interest to serve by making the severity of small-pox large or small, gives an average of from 14 to 18 per cent.5 as the proportion of small-pox deaths to cases; and we naturally ask, How is it that, with so much better sanitary conditions and greatly improved treatment, nearly half the unvaccinated patients die, while in the last century less than one-fifth died? Many of the supporters of vaccination, such as Dr. Gayton (2nd Rep., p. 1856), have no explanation to offer. Others, such as Dr. Whitelegge (6th Rep., p. 533), believe that small-pox becomes more virulent periodically, and that one of its maxima of virulence caused the great epidemic of 1870-72, which, after more than half a century of vaccination equalled some of the worst epidemics of the pre-vaccination period. It is, however, a most suggestive fact that, considering small-pox mortality per se, without reference to vaccination–the records of which are, as have been shown, utterly untrustworthy–We find the case-mortality to agree closely with that of the last century. Thus the figures given in the Reports of the Hampstead, Homerton, and Deptford small-pox hospitals at periods between 1876 and 1879 were, 19, 18.8, and 17 per cent. respectively (3rd Report, p. 205). If we admit that only the worst cases went to the hospitals, but also allow something for better treatment now, the result is quite explicable; whereas the other result, of a greatly increased fatality in the unvaccinated so exactly balanced by an alleged greatly diminished fatality in the vaccinated is not explicable, especially when we remember that this diminished fatality applies to all ages, and it is now almost universally admitted that the alleged protective influence of vaccination dies out in ten or twelve years. These various opinions are really self-destructive. If epidemic small-pox is now much more virulent than in the last century, as shown by the greater mortality of [[p. 29]] the unvaccinated now than then, the greatly diminished or almost vanishing effect of primary vaccination in adults cannot possibly have reduced their fatality to one-fifth or one-sixth of that of the other class. Again, it is admitted by many pro-vaccinist authorities that the unvaccinated, as a rule, belong to the poorer classes, while they also include most of the criminal classes, tramps, and generally the nomad population. They also include all those children whose vaccination has been deferred on account of weakness, or of their suffering from other diseases, as well as all those under vaccination age. The unvaccinated as a class are therefore especially liable to zymotic disease of any kind, small-pox included; and when, in addition to these causes of a higher death-rate from small-pox, we take account of the proved untrustworthiness of the statistics, wholly furnished by men who are prejudiced in favour of vaccination (as instanced by the declaration of Dr. Gayton, that when the eruption is so severe as on the third day to hide the vaccination marks, it affords primâ facie evidence of non-vaccination (2nd Report, Q. 1790), we are fully justified in rejecting all arguments in favour of vaccination supported by such fallacious evidence. And this is the more rational course to be adopted by all unprejudiced enquirers, because, as I shall now proceed to show, there is an abundance of facts of a more accurate and more satisfactory nature by which to test the question.6 One more point may be referred to before quitting this part of the subject, which is, that the more recent official hospital-statistics themselves afford a demonstration of the non-protective influence of vaccination, and thus [[p. 30]] serve as a complete refutation of the conclusions drawn from the statistics we have just been dealing with. Dr. Munk stated before the Hospital Commission, that the percentage of vaccinated patients in the London small-pox hospital had increased from 40 per cent. in 1838 to 94 6/10 per cent. in 1879 (3rd Report of Royal Comm., Q. 9090). This evidence was given in 1882; but Mr, Wheeler stated that according to the Reports of the Highgate hospital, the vaccinated patients had long been over 90 per cent. of the whole, and are now often even 94 or 95 per cent. The hospitals of the Metropolitan Asylums Board, which take in mostly pauper patients, give a lower percentage–the Homerton hospital 85 per cent., the Deptford hospital 87 per cent., and the Hampstead hospital 75 per cent.–in the two latter cases adding the “doubtful” class to the vaccinated, as the facts already given prove that we have a right to do and still probably give too high a proportion of unvaccinated. As the proportion of the London population that is vaccinated cannot be over 90 per cent. (see Minority Report, pp. 173-4), and is probably much lower, and considering the kind of patients the unvaccinated include (see back, p. 29), there remains absolutely nothing for the effects of vaccination. We have already seen that the total case-mortality of these hospitals agrees closely with that of the last century; the two classes of facts taken together thus render it almost certain that vaccination has never saved a single human life. [[p. 31]] CHAPTER III THE GENERAL STATISTICS OF SMALL-POX MORTALITY IN RELATION TO VACCINATION Having thus cleared away the mass of doubtful or erroneous statistics depending on comparisons of the vaccinated and the unvaccinated in limited areas or selected groups of patients, we turn to the only really important evidence, those “masses of national experience” which Sir John Simon, the great official advocate of vaccination, tells us we must now appeal to for an authoritative decision on the question of the value of vaccination; to which may be added certain classes of official evidence serving as test cases or “control experiments” on a large scale. Almost the whole of the evidence will be derived from the Reports of the recent Royal Commission. In determining what statistics really mean the graphic is the only scientific method, since, except in a few very simple cases, long tables of figures are confusing; and if divided up and averages taken, as is often done, they can be manipulated so as to conceal their real teaching. Diagrams, on the other hand, enable us to see the whole bearing of the variations that occur, while for comparisons of one set of figures with another their superiority is overwhelming. This is especially the case with the statistics of epidemics and of general mortality, because the variations are so irregular and often so large as to render tables of figures very [[p. 32]] puzzling, while any just comparison of several tables with each other becomes impossible. I shall therefore put all the statistics I have to lay before my readers in the form of diagrams, which, I believe, with a little explanation, will enable any one to grasp the main points of the argument. LONDON MORTALITY AND SMALL-POX The first and largest of the diagrams illustrating this question is that exhibiting the mortality of London from the year 1760 down to the present day (see end of volume). It is divided into two portions, that from 1750 to 1834 being derived from the old “Bills of Mortality,” that from 1838 to 1896 from the Reports of the Registrar-General. The “Bills of Mortality” are the only material available for the first period, and they are far inferior in accuracy to the modern registration, but they are probably of a fairly uniform character throughout, and may therefore be as useful for purposes of comparison as if they were more minutely accurate. It is admitted that they did not include the whole of the deaths, and the death-rates calculated from the estimated population will therefore be too low as compared with those of the Registrar-General, but the course of each death rate–its various risings or failings–will probably be nearly true.7 The years are given along the bottom of the diagram, and the deaths per million [[p. 33]] living are indicated at the two ends and in the centre, the last four years of the Bills of Mortality being omitted because they are considered to be especially inaccurate. The upper line gives the total death-rate from all causes, the middle line the death-rate from the chief zymotic diseases–measles, scarlet-fever, diphtheria, whooping-cough and, fevers generally, excluding small-pox, and the lower line small-pox only. The same diseases, as nearly as they can be identified in the Bills of Mortality according to Dr. Creighton, are given in the earlier portion of the diagram from the figures given in his great work, A History of Epidemics in Britain. With the exception of these zymotics the diagram is the same as that presented to the Royal Commission (3rd Report, diagram J.), but it is carried back to an earlier date. Let us now examine the lowest line, showing the small-pox death-rate. First taking the period from 1760 to 1800, we see, amid great fluctuations and some exceptional epidemics, a well-marked steady decline which, though obscured by its great irregularity, amounts to a difference of 1,000 per million living. This decline continues, perhaps somewhat more rapidly, to 1820. From that date to 1834 the decline is much less, and is hardly perceptible. The period of Registration opens with the great epidemic of 1838, and thenceforward to 1885 the decline is very slow indeed; while, if we average the great epidemic of 1871 with the preceding ten years, we shall not be able to discover any decline at all. From 1886, however, there is a rather sudden decline to a very low death-rate, which has continued to the present time. Now it is alleged by advocates of vaccination, and by the Commissioners in their Report, that the decline from 1800 onwards is due to vaccination, either wholly or in great part, and that “the marked decline of small-pox in the first quarter of the present century affords substantial evidence in favour of the protective influence of vaccination.”8 This conclusion is not only entirely [[p. 34]] unwarranted by the evidence on any accepted methods of scientific reasoning, but it is disproved by several important facts. In the first place the decline in the first quarter of the century is a clear continuation of a decline which had been going on during the preceding forty years, and whatever causes produced that earlier decline may very well have produced the continuation of it. Again, in the first quarter of the century, vaccination was comparatively small in amount and imperfectly performed. Since 1854 it has been compulsory and almost universal; yet from 1854 to 1884 there is almost no decline of small-pox perceptible, and the severest epidemic of the century occurred in the midst of that period. Yet again, the one clearly marked decline of small-pox has been in the ten years from 1886 to 1896, and it is precisely in this period that there has been a great falling off in vaccination in London from only 7 per cent. less than the births in 1885 to 20.6 per cent. less in 1894, the last year given in the Reports of the Local Government Board; and the decrease of vaccinations has continued since. But even more important, as showing that vaccination has had nothing whatever to do with the decrease of small-pox, is the very close general parallelism of the line showing the other zymotic diseases, the diminution of which it is admitted has been caused by improved hygienic conditions. The decline of this group of diseases in the first quarter of this century, though somewhat less regular, is quite as well marked as in the case of small-pox, as is also its decline in the last forty years of the 18th century, strongly suggesting that both declines are due to common causes. Let any one examine this diagram carefully and say if it is credible that from 1760 to 1800 both declines are due to some improved conditions of hygiene and sanitation, but that after 1800, while the zymotics have continued to decline from the same class of causes one zymotic–small-pox–must have been influenced by a new cause–vaccination, to produce its corresponding decline. Yet this is the astounding claim made by [[p. 35]] the Royal Commissioners! And if we turn to the other half of the diagram showing the period of registration, the difficulty becomes even greater. We first have a period from 1838 to 1870, in which the zymotics actually rose; and from 1838 to 1871, averaging the great epidemic with the preceding ten years, we find that small-pox also rose, or at the best remained quite stationary. From 1871 to 1875 zymotics are much lower, but run quite parallel with small-pox; then there is a slight decline in both, and zymotics and small-pox remain lower in the last ten years than they have ever been before, although in this last period vaccination has greatly diminished. Turning to the upper line, showing the death-rate from all causes, we again find a parallelism throughout, indicating improved general conditions acting upon all diseases. The decline of the total death-rate from 1760 to 1810 is remarkably great, and it continues at a somewhat less rate to 1830, just as do the zymotics and small-pox. Then commences a period from 1840 to 1870 of hardly perceptible decline partly due to successive epidemics of cholera, again running parallel with the course of the zymotics and of small-pox, followed by a great decline to the present time, corresponding in amount to that at the beginning of the century. The Commissioners repeatedly call attention to the fact that the mortality from measles has not at all declined and that other zymotics have not declined in the same proportion as small-pox, and they argue: “If improved sanitary conditions were the cause of small-pox becoming less, we should expect to see that they had exercised a similar influence over almost all other diseases. Why should they not produce the same effect in the case of measles, scarlet fever, whooping-cough, and indeed any disease spread by contagion or infection and from which recovery was possible?” This seems a most extraordinary position to be taken in view of the well-known disappearance of various diseases at different epochs. Why did leprosy almost [[p. 36]] disappear from England at so early a period and plague later on? Surely to some improved conditions of health. The Commissioners do not, and we may presume cannot, tell us why measles, of all the zymotic diseases, has rather increased than diminished during the whole of this century. Many students of epidemics hold that certain diseases are liable to replace each other, as suggested by Dr. Watt, of Glasgow, in the case of measles and small-pox. Dr. Farr, the great medical statistician, adopted this view. In his Annual Report to the Registrar-General in l872 (p. 224), he says: “The zymotic diseases replace each other; and when one is rooted out it is apt to be replaced by others which ravage the human race indifferently whenever the conditions of healthy life are wanting. They have this property in common with weeds and other forms of life: as one species recedes another advances.” This last remark is very suggestive in view of the modern germ-theory of these diseases. This substitution theory is adopted by Dr. Creighton, who in his History of Epidemics in England suggests that plague was replaced by typhus fever and small-pox; and, later on, measles, which was insignificant before the middle of the seventeenth century, began to replace the latter disease. In order to show the actual state of the mortality from these diseases during the epoch of registration, I have prepared a diagram (II.) giving the death-rates for London of five of the chief zymotics, from the returns of the Registrar-General, under the headings he adopted down to 1868–for to divide fevers into three kinds for half the period, and to separate scarlatina and diphtheria, as first done in 1859, would prevent any useful comparison from being made. The lowest line, as in the larger diagram, shows Small-pox. Above it is Measles, which keeps on the whole a very level course, showing, however, the high middle period of the zymotics and two low periods, from 1869 to 1876, and from 1848 to 1856, the first nearly corresponding to the very high small-pox [[p. 37]] death-rate from 1870 to 1881; and the other just following the two small-pox epidemics of 1844 and 1848, thus supporting the view that it is in process of replacing that disease. Scarlatina and diphtheria show the high rate of zymotics generally from 1848 to 1870, with a large though irregular decline subsequently. Whooping-cough shows a nearly level course to 1882 and then a well-marked decline. Fevers (typhus, enteric, and simple) show the usual high middle period, but with an earlier and more continuous decline than any of the other zymotic diseases. We thus see that all these diseases exhibit common features though in very different degrees, all indicating the action of general causes, some of which it is by no means difficult to point out. In 1845 began the great development of our railway system, and with it the rapid growth of London, from a population of two millions in 1844 to one of four millions in 1884. This rapid growth of population was at first accompanied with over-crowding, and as no adequate measures of sanitation were then provided the conditions were prepared for that increase of zymotic disease which constitutes so remarkable a feature of the London death-rates between 1848 and 1866. But at the latter date commenced a considerable decline both in the total mortality and in that from all the zymotic diseases, except measles and small-pox, but more especially in fevers and diphtheria, and this decrease is equally well explained by the completion, in 1865, of that gigantic work, the main drainage of London. The last marked decline in small-pox, in fevers, and to a less marked degree in whooping-cough, is coincident with a recognition of the fact that hospitals are themselves often centres of contagion, and the establishment of floating hospitals for London cases of small-pox. Perhaps even more beneficial was the modern system of excluding sewer-gas from houses. We thus see that the increase or decrease of the chief zymotic diseases in London during the period [[p. 38]] of registration is clearly connected with adverse or favourable hygienic conditions of a definite kind. During the greater part of this period small-pox and measles alone showed no marked increase or decrease, indicating that the special measures affecting them had not been put in practice, till ten years back the adoption of an effective system of isolation in the case of small-pox has been followed by such marked results wherever it has been adopted as to show that this is the one method yet tried that has produced any large and unmistakable effect, thus confirming the experience of the town of Leicester, which will be referred to later on. The Commissioners in their Final Report lay the greatest stress on the decline of small-pox at the beginning of the century, which “followed upon the introduction of vaccination,” both in England, in Western Europe, and in the United States. They declare that “there is no proof that sanitary improvements were the main cause of the decline of small-pox,” and that “no evidence is forthcoming to show that during the first quarter of the nineteenth century these improvements differentiated that quarter from the last quarter or half of the preceding century in any way at all comparable to the extent of the differentiation in respect to small-pox” (p. 19 par. 79). To the accuracy of these statements I demur in the strongest manner. There is proof that sanitary improvements were the main cause of this decline of small-pox early in the century, viz., that the other zymotic diseases as a whole showed a simultaneous decline to a nearly equal amount, while the general death-rate showed a decline to a much greater amount, both admittedly due to improved hygienic conditions, since there is no other known cause of the diminution of disease; and that the Commissioners altogether ignore these two facts affords, to my mind, a convincing proof of their incapacity to deal with this great statistical question. And, as to the second point, I maintain that there is ample direct evidence, [[p. 39]] for those who look for it, of great improvements in the hygienic conditions of London quite adequate to account for the great decline in the general mortality, and therefore equally adequate to account for the lesser declines in zymotic diseases and in small-pox, both of which began in the last century, and only became somewhat intensified in the first quarter of the present century, to be followed twenty years later by a complete check or even a partial rise. This rise was equally marked in small-pox as in the other diseases, and thus proved, as clearly as anything can be proved, that its decline and fluctuations are in no way dependent on vaccination, but are due to causes of the very same general nature as in the case of other diseases. To give the evidence for this improvement in London hygiene would, however, break the continuity of the discussion as to small-pox and vaccination; but the comparison of the general and zymotic death-rates with that of small-pox exhibits so clearly the identity of the causes which have acted upon them all as to render the detailed examination of the various improved conditions that led to the diminished mortality unnecessary. The diagram showing the death-rates from these three causes of itself furnishes a complete refutation of the Commissioners’ argument. The evidence as to the nature of the improved conditions will be given in another work to be published shortly. SMALL-POX AND OTHER DISEASES IN BRITAIN DURING THE PERIOD OF REGISTRATION We have no general statistics of mortality in England and Wales till the establishment of the Registration system in 1838, but the results make up for their limited duration by their superior accuracy. Till the year 1870 no record was kept of the amount of vaccination except as performed by the public vaccinators, but since 1872 all vaccinations are [[p. 40]] recorded, and the numbers published by the Local Government Board. My third diagram is for the purpose of showing graphically the relation of small-pox to other zymotic diseases, and to vaccination, for England and Wales. The lower line shows small-pox, the middle one zymotic diseases, and the upper the total death-rates. The relations of the three are much the same as in the London diagram, the beginning of the great decline of zymotics being in 1871, and that of small-pox in 1872, but the line of small-pox is much lower, and zymotics somewhat lower than in London, due to a larger proportion of the inhabitants living under comparatively healthy rural conditions. But if the amount of vaccination were the main and almost exclusive factor in determining the amount of small-pox, there ought to be little or no difference between London and the country. But here, as in all other cases, the great factor of comparative density of population in compared areas is seen to have its full effect on small-pox mortality as in that of all other zymotic diseases. This non-relation between vaccination and small-pox mortality is further proved by the thick dotted line showing the vaccinations per cent. of births for the last 22 years, as given in the “Final Report” (p. 34). The diminution of vaccination in various parts of the country began about 1884, and from 1886 has been continuous and rapid, and it is during this very period that small-pox has been continuously less in amount than has ever been known before. Both in the relation of London small-pox to that of the whole country, and in the relation of small-pox to vaccination, we find proof of the total inefficacy of that operation. SMALL-POX IN SCOTLAND AND IN IRELAND In their Final Report the Commissioners give us Tables of the death-rates from small-pox, measles, and scarlet-fever in Scotland and Ireland; and from these [[p. 41]] Tables I have constructed my diagram (IV.), combining the two latter diseases for simplicity, and including the period of compulsory vaccination and accurate registration in both countries. The most interesting feature of this diagram is the striking difference in the death-rates of the two countries. Scotland, the richer, more populous, and more prosperous country having a much greater mortality, both from the two zymotics and from small-pox, than poor, famine-stricken, depopulated Ireland. The maximum death-rate by the two zymotics in Scotland is considerably more than double that in Ireland, and the minimum is larger in the same proportion. In small-pox the difference is also very large in the same direction, for although the death-rate during the great epidemic in 1872 was only one-fourth greater in Scotland, yet as the epidemic there lasted three years, the total death-rate for those years was nearly twice as great as for the same period in Ireland, which, however, had a small epidemic later on in 1878. Since 1883 small-pox has been almost absent from both countries, as from England; but taking the twenty years of repeated epidemics from 1864 to 1883, we find the average small-pox death-rate of Scotland to be about 139, and that of Ireland 85 per million, or considerably more than as three to two. But even Scotland had a much lower small-pox mortality than England, the proportions being as follows for the three years which included the epidemic of 1871-3: Ireland, 800 per million in the three years. Now the Royal Commissioners make no remark whatever on these very suggestive facts, and they have arranged the information in tables in such a way as to render it very difficult to discover them; and this is another proof of their incapacity to deal with statistical questions. They seem to be unable to [[p. 42]] look at small-pox from any other point of view than that of the vaccinationist, and thus miss the essential features of the evidence they have before them. Every statistician knows the enormous value of the representation of tabular statistics by means of diagrammatic curves. It is the only way by which in many cases the real teaching of statistics can be detected. An enormous number of such diagrams, more or less instructive and complete, were presented to them, and, at great cost, are printed in the Reports; but I cannot find that, in their Final Report, they have made any adequate use of them, or have once referred to them, and thus it is that they have overlooked so many of the most vital teachings of the huge mass of figures with which they had to deal. It is one of the most certain of facts relating to sanitation that comparative density of population affects disease, and especially the zymotic diseases, more than any other factor that can be ascertained. It is mainly a case of purity of the air, and consequent purification of the blood; and when we consider that breathing is the most vital and most continuous of all organic functions, that we must and do breathe every moment of our lives, that the air we breathe is taken into the lungs, one of the largest and most delicate organs of the body, and that the air so taken in acts directly upon the blood, and thus affects the whole organism, we see at once how vitally important it is that the air around us should be as free as possible from contamination, either by the breathing of other people, or by injurious gases or particles from decomposing organic matter, or by the germs of disease. Hence it happens that under our present terribly imperfect social arrangements the death-rate (other things being equal) is a function of the population per square mile, or perhaps more accurately of the proportion of town to rural populations. In the light of this consideration let us again compare these diagrams of Irish, Scottish, and English death-rates. In Ireland only 11 per cent. of the [[p. 43]] population live in the towns of 100,000 inhabitants and upwards. In Scotland 30 per cent., and in England and Wales 54 per cent.; and we find the mortality from zymotic diseases to be roughly proportional to these figures. We see here unmistakable cause and effect. Impure air, with all else that overcrowding implies on the one hand, higher death-rate on the other. This explains the constant difference between London and rural mortality, and it also explains what seems to have puzzled the Commissioners more than anything else–the intractability of some of the zymotics to ordinary sanitation, as in the case of measles especially, and in a less degree of whooping-cough–for in their case the continual growth of urban as opposed to rural populations has neutralised the effects of such improved conditions as we have been able to introduce. But the most important fact for our present purpose is, that small-pox is subject to this law just as are the other zymotics, while it pays no attention whatever to vaccination. The statistician to the Registrar-General for Scotland gave evidence that ever since 1864 more than 96 per cent. of the children born have been vaccinated or had had previous small-pox, and he makes no suggestion of any deficiency that can be remedied. But in the case of Ireland the medical commissioner for the Local Government Board for Ireland, Dr. MacCabe, told the Commissioners that vaccination there was very imperfect, and that a large proportion of the population was “unprotected by vaccination,” this state of things being due to various causes, which he explained (2nd Rep., QQ. 3,059-3,075). But neither Dr. MacCabe nor the Commissioners notice the suggestive, and from their point of view alarming, fact that imperfectly vaccinated Ireland had had far less small-pox mortality than thoroughly well-vaccinated Scotland, enormously less than well-vaccinated England, and overwhelmingly less than equally well-vaccinated London. Ireland–Scotland–England–London–a graduated series in density of [[p. 44]] population, and in zymotic death-rate; the small-pox death-rate increasing in the same order and to an enormous extent, quite regardless of the fact that the last three have had practically complete vaccination during the whole period of the comparison; while Ireland alone, with the lowest small-pox death-rate by far, has, on official testimony, the least amount of vaccination. And yet the majority of the Commissioners still pin their faith on vaccination, and maintain that the cumulative force of the testimony in its favour is irresistible! And further, that “sanitary improvements” cannot be asserted to afford “an adequate explanation of the diminished mortality from small-pox.” It will now be clear to my readers that these conclusions, set forth as the final outcome of their seven years’ labours, are the very reverse of the true ones, and that they have arrived at them by neglecting altogether to consider, in their mutual relations, “those great masses of national statistics” which alone can be depended on to point out true causes, but have limited themselves to such facts as the alleged mortalities of the vaccinated and the unvaccinated, changes of age-incidence, and other matters of detail, some of which are entirely vitiated by untrustworthy evidence while others require skilled statistical treatment to arrive at true results, a subject quite beyond the powers of untrained physicians and lawyers, however eminent in their own special departments.9 SMALL-POX AND VACCINATION ON THE CONTINENT Before proceeding to discuss those special test-cases in our own country which still more completely show the impotence of vaccination, it will be well to notice [[p. 45]] a few Continental States which have been, and still are, quoted as affording illustrations of its benefits. We will first take Sweden, which has had fairly complete national statistics longer than any other country, and we are now fortunately able to give the facts on the most recent official testimony–the Report furnished by the Swedish Board of Health to the Royal Commission, and published in the Appendix to their Sixth Report (pp. 751-56). Such great authorities as Sir William Gull, Dr. Seaton, and Mr. Marson, stated before the Committee of Enquiry in 1871 that Sweden was one of the best vaccinated countries, and that the Swedes were the best vaccinators. Sir John Simon’s celebrated paper, which was laid before Parliament in 1857 and was one of the chief supports of compulsory legislation, made much of Sweden, and had a special diagram to illustrate the effects of vaccination on small-pox. This paper is reproduced in the First Report of the recent Royal Commission (pp. 61-113), and we find the usual comparison of small-pox mortality in the last and present century which is held to be conclusive as to the benefits of vaccination. He says vaccination was introduced in 1801, and divides his diagram into two halves differently coloured before and after this date. It will be observed that, as in England, there was a great and sudden decrease of small-pox mortality after 1801, the date of the first vaccination in Sweden, and by 1812 the whole reduction of mortality was completed. But from that date for more than sixty years there was an almost continuous increase in frequency and severity of the epidemics. To account for this sudden and enormous decrease Sir John Simon states, in a note, and without giving his authority: “About 1810 the vaccinations were amounting to nearly a quarter of the number of births.” But these were almost certainly both adults and children of various ages, and the official returns now given show that down to 1812, when the whole reduction of small-pox mortality had been effected, only 8 per cent. of the population had been vaccinated. We [[p. 46]] are told in a note to the official tables that the first successful vaccination in Stockholm was at the end of 1810, so that the earlier vaccinations must have been mainly in the rural districts; yet the earlier Stockholm epidemics in 1807, before a single inhabitant was vaccinated, and in 1825, were less severe than the six later ones, when vaccination was far more general. Bearing these facts in mind, and looking at diagram V., we see that it absolutely negatives the idea of vaccination having had anything to do with the great reduction of small-pox mortality, which was almost all effected before the first successful vaccination in the capital on the 17th December, 1810! And this becomes still more clear when we see that as vaccination increased among a population which, the official Report tells us, had the most “perfect confidence” in it, small-pox epidemics increased in virulence, especially in the capital (shown in the diagram by the dotted peaks) where, in 1874, there was a small-pox mortality of 7,916 per million, reaching 10,290 per million during the whole epidemic, which lasted two years. This was worse than the worst epidemic in London during the eighteenth century.10 But although there is no sign of a relation between vaccination and the decrease of small-pox, there is a very clear relation between it and the decrease in the general mortality. This is necessarily shown on a much smaller vertical scale to bring it into the diagram. If it were on the same scale as the small-pox line, its downward slope would be four times as rapid as it is. The decrease in the century is from about 27,000 to 15,000 per million, and, with the exception of the period of the Napoleonic wars, the improvement is nearly continuous throughout. There has evidently been a great and continuous improvement in healthy conditions of life in Sweden, as in our own country [[p. 47]] and probably in all other European nations; and this improvement, or some special portion of it, must have acted powerfully on small-pox to cause the enormous diminution of the disease down to 1812, with which, as we have seen, vaccination could have had nothing to do. The only thing that vaccination seems to have done is, to have acted as a check to this diminution, since it is otherwise impossible to explain the complete cessation of improvement as the operation became more general; and this is more especially the case in view of the fact that the general death-rate has continued to decrease at almost the same rate down to the present day! The enormous small-pox mortality in Stockholm has been explained as the result of very deficient vaccination; but the Swedish Board of Health states that this deficiency was more apparent than real, first, because 25 per cent. of the children born in Stockholm die before completing their first year, and also because of neglect to report private vaccinations, so that “the low figures for Stockholm depend more on the cases of vaccination not having been reported than on their not having been effected.” (Sixth Report, p. 754, 1st col., 3rd par.) The plain and obvious teaching of the facts embodied in this diagram is, that small-pox mortality is in no way influenced (except it be injuriously) by vaccination, but that here, as elsewhere, it does bear an obvious relation to density of population; and also that, when uninfluenced by vaccination, it follows the same law of decrease with improved conditions of general health as does the total death-rate. This case of Sweden alone affords complete proof of the uselessness of vaccination; yet the Commissioners in the Final Report (par. 59) refer to the great diminution of small-pox mortality in the first twenty years of the century as being due to it. They make no comparison with the total death-rate; they say nothing of the increase of small-pox from 1824 to 1874; they omit all reference to the terrible Stockholm epidemics [[p. 48]] increasing continuously for fifty years of legally enforced vaccination and culminating in that of 1874, which was far worse than the worst known in London during the whole of the eighteenth century. Official blindness to the most obvious facts and conclusions can hardly have a more striking illustration than the appeal to the case of Sweden as being favourable to the claims of vaccination. My next diagram (No. VI.) shows the course of small-pox in Prussia since 1816, with an indication of the epidemics in Berlin in 1864 and 1871. Dr. Seaton, in 1871, said to the Committee on Vaccination (Q. 5,608), “I know Prussia is well protected,” and the general medical opinion was expressed thus in an article in the Pall Mall Gazette (May 24, 1871): “Prussia is the country where revaccination is most generally practised, the law making the precaution obligatory on every person, and the authorities conscientiously watching over its performance. As a natural result, cases of small-pox are rare.” Never was there a more glaring untruth than this last statement. It is true that revaccination was enforced in public schools and other institutions, and most rigidly in the Army, so that a very large proportion of the adult male population must have been revaccinated; but, instead of cases of small-pox being rare, there had been for the twenty-four years preceding 1871 a much greater small-pox mortality in Prussia than in England, the annual average being 248 per million for the former and only 210 for the latter. A comparison of the two diagrams shows the difference at a glance. English small-pox only once reached 400 per million (in 1852), while in Prussia it four times exceeded that amount. And immediately after the words above quoted were written the great epidemic of 1871-72 caused a mortality in revaccinated Prussia more than double that of England! Now, after these facts have been persistently made known by the anti-vaccinators, the amount of vaccination in Prussia before 1871 is depreciated, and Dr. A. F. Hopkirk actually classes it [[p. 49]] among countries “without compulsory vaccination.” (See table and diagram opposite p. 238 in the 2nd Report.) In the city of Berlin we have indicated two epidemics, that in 1864, with a death-rate a little under 1,000 per million, while that in 1871 rose to 6,150 per million, or considerably more than twice as much as that of London in the same year, although the city must have contained a very large male population which had passed through the army, and had therefore been revaccinated. I give one more diagram (No. VII.) of small-pox in Bavaria, from a table laid before the Royal Commission by Dr. Hopkirk for the purpose of showing the results of long-continued compulsory vaccination. He stated to the Commission that vaccination was made compulsory in 1807, and that in 1871 there were 30,742 cases of small-pox, of which 95.7 per cent. were vaccinated. (2nd Report, Q. 1,489.) He then explains that this was because “nearly the whole population was vaccinated”; but he does not give any figures to prove that the vaccinated formed more than this proportion of the whole population; and as the vaccination age was one year, it is certain that they did not do so.11 He calls this being “slightly attacked,” and argues that it implies “some special protection.” No doubt the small-pox mortality of Bavaria was rather low, about equal to that of Ireland; but in 1871 it rose to over 1,000 per million, while Ireland had only 600, besides which the epidemic lasted for two years, and was therefore very nearly equal to that of England. But we have the explanation when we look at the line showing the other zymotics, for these are decidedly lower than those of England, showing better general sanitary conditions. In Bavaria, as in all the other countries we have examined, the behaviour of small-pox shows no relation to vaccination, but the very [[p. 50]] closest relation to the other zymotics and to density of population. The fact of 95.7 per cent. of the small-pox patients having been vaccinated agrees with that of our Highgate hospital, but is even more remarkable as applying to the population of a whole country, and is alone sufficient to condemn vaccination as useless. And as there were 5,070 deaths to these cases, the fatality was 16.5 per cent., or almost the same as that of the last century; so that here again, and on a gigantic scale, the theory that the disease is “mitigated” by vaccination, even where not prevented, is shown to be utterly baseless. Yet this case of Bavaria was chosen by a strong vaccinist as affording a striking proof of the value of vaccination when thoroughly carried out, and I cannot find that the Commissioners took the trouble to make the comparisons here given, which would at once have shown them that what the case of Bavaria really proves is the complete uselessness of vaccination. This most misleading, unscientific, and unfair proceeding, of giving certain figures of small-pox mortality among the well vaccinated, and then, without any adequate comparison, asserting that they afford a proof of the value of vaccination, may be here illustrated by another example. In the original paper by Sir John Simon on the History and Practice of Vaccination, presented to Parliament in 1857, there is, in the Appendix, a statement by Dr. T. Graham Balfour, surgeon to the Royal Military Asylum for Orphans at Chelsea, as to the effects of vaccination in that institution–that since the opening of the Asylum in 1803 the Vaccination Register has been accurately kept, and that every one who entered was vaccinated unless he had been vaccinated before or had had small-pox; and he adds: “Satisfactory evidence can therefore, in this instance, be obtained that they were all protected.” Then he gives the statistics, showing that during forty-eight years, from 1803 to 1851, among 31,705 boys there were thirty-nine cases and four deaths, giving a mortality at the rate of 126 per [[p. 51]]million on the average number in the Asylum, and concludes by saying: “The preceding facts appear to offer most conclusive proofs of the value of vaccination.” But he gives no comparison with other boys of about the same age and living under equally healthy conditions, but who had not been so uniformly or so recently vaccinated; for it must be remembered that, as this was long before the epoch of compulsory vaccination, a large proportion of the boys would be unvaccinated at their entrance, and would therefore have the alleged benefit of a recent vaccination. But when we make the comparison, which both Dr. Balfour and Sir John Simon failed to make, we find that these well vaccinated and protected boys had a greater small-pox mortality than the imperfectly protected outsiders. For in the First Report of the Commission (p. 114, Table B) we find it stated that in the period of optional vaccination (1847-53) the death-rate from small-pox of persons from ten to fifteen years12 was 94 per million! Instead of offering “most conclusive proofs of the value of vaccination,” his own facts and figures, if they prove anything at all, prove not only the uselessness but the evil of vaccination, and that it really tends to increasesmall-pox mortality. And this conclusion is also reached by Professor Adolf Vogt, who, in the elaborate statistical paper sent by him to the Royal Commission, and printed in their Sixth Report, but not otherwise noticed by them, shows by abundant statistics from various countries that the small-pox death-rate and fatality have been increased during epidemics occurring in the epoch of vaccination. One more point deserves notice before leaving this part of the inquiry, which is the specially high small-pox mortality of great commercial seaports. The following table, compiled from Dr. Pierce’s Vital Statistics for the Continental towns and from the [[p. 52]]Reports of the Royal Commission for those of our own country, is very remarkable and instructive. Name of Town . . . . . Year . . . . . Small-pox Death-rate per Million The small-pox death-rate in the case of the lowest of these towns is very much higher than in London during the same epidemic, and it is quite clear that vaccination can have had nothing to do with this difference. For if it be alleged that vaccination was neglected in Hamburgh and Rotterdam, of which we find no particulars, this cannot be said of Cork, Sunderland, and Newcastle. Again, if the very limited and imperfect vaccination of the first quarter of the century is to have the credit of the striking reduction of small-pox mortality that then occurred, as the Royal Commissioners claim, a small deficiency in the very much more extensive and better vaccination that generally prevailed in 1871, cannot be the explanation of a small-pox mortality greater than in the worst years of London when there was no vaccination. Partial vaccination cannot be claimed as producing marvellous effects at one time and less than nothing at all at another time, yet this is what the advocates of vaccination constantly do. But on the sanitation theory the explanation is simple. Mercantile seaports have grown up along the banks of harbours or tidal rivers whose waters and shores have been polluted by sewage [[p. 53]] for centuries. They are always densely crowded owing to the value of situations as near as possible to the shipping. Hence there is always a large population living under the worst sanitary conditions, with bad drainage, bad ventilation, abundance of filth and decaying organic matter, and all the conditions favourable to the spread of zymotic diseases and their exceptional fatality. Such populations have maintained to our day the insanitary conditions of the last century, and thus present us with a similarly great small-pox mortality, without any regard to the amount of vaccination that may be practised. In this case they illustrate the same principle which so well explains the very different amounts of small-pox mortality in Ireland, Scotland, England, and London, with hardly any difference in the quantity of vaccination. The Royal Commissioners, with all these facts before them or at their command, have made none of these comparisons. They give the figures of small-pox mortality, and either explain them by alleged increase or decrease of vaccination, or argue that, as some other disease–such as measles–did not decrease at the same time or to the same amount, therefore sanitation cannot have influenced small-pox. They never once compare small-pox mortality with general mortality, or with the rest of the group of zymotics, and thus fail to see their wonderfully close agreement–their simultaneous rise and fall, which so clearly shows their subjection to the same influences and proves that no special additional influence can have operated in the case of small-pox. [[p. 54]] CHAPTER IV TWO GREAT EXPERIMENTS WHICH ARE CONCLUSIVE AGAINST VACCINATION Those who disbelieve in the efficacy of vaccination to protect against small-pox are under the disadvantage that, owing to the practice having been so rapidly adopted by all civilized people, there are no communities who have rejected it while adopting methods of general sanitation, and who have also kept satisfactory records of mortality from various causes. Any such country would have afforded what is termed a “control” or test experiment, the absence of which vitiates all the evidence of the so-called “variolous test” in Jenner’s time, as was so carefully pointed out before the Commission by Dr. Creighton and Professor Crookshank. We do, however, now possess two such tests on a limited, but still a sufficient scale. The first is that of the town of Leicester, which for the last twenty years has rejected vaccination till it has now almost vanished altogether. The second is that of our Army and Navy, in which, for a quarter of a century, every recruit has been revaccinated, unless he has recently been vaccinated or has had small-pox. In the first we have an almost wholly “unprotected” population of nearly 200,000, which, on the theory of the vaccinators, should have suffered exceptionally [[p. 55]] from small-pox; in the other we have a picked body of 220,000 men, who, on the evidence of the medical authorities, are as well protected as they know how to make them, and among whom, therefore, small-pox should be almost or quite absent, and small-pox deaths quite unknown. Let us see, then, what has happened in these two cases. Perhaps the most remarkable and the most complete body of statistical evidence presented to the Commission was that of Mr. Thomas Biggs, a sanitary engineer and a town councillor of Leicester. It consists of fifty-one tables exhibiting the condition of the population in relation to health and disease from almost every conceivable point of view. The subject is further illustrated by sixteen diagrams, many of them in colours, calculated to exhibit to the eye in the most clear and simple manner the relations of vaccination and sanitation to small-pox and to the general health of the people, and especially of the children, in whose behalf it is always alleged vaccination is enforced. From this wealth of material I can give only two diagrams exhibiting the main facts of the case, as shown by Mr. Biggs’ statistics in the Fourth Report of the Royal Commission, all obtained from official sources. The first diagram (No. VIII.) shows in the upper part, by a dotted line, the total vaccinations, public and private, since 1850.13 The middle line shows the mortality per million living from the chief zymotic diseases–fevers, measles, hooping-cough, and diphtheria–while the lower line gives the small-pox mortality. We notice here a high mortality from zymotics and from small-pox epidemics, during the whole period of nearly complete vaccination from 1854 to 1870. Then commenced the movement against vaccination, owing to its proved uselessness in the great epidemic when Leicester had a very much higher [[p. 56]] small-pox mortality than London, which has resulted in a continuous decline, especially rapid for the last fifteen years, till it is now reduced to almost nothing. For that period not only has small-pox mortality been continuously very low, but the zymotic diseases have also regularly declined to a lower amount than has ever been known before. The second diagram (No. IX.) is even more important, as showing the influence of vaccination in increasing both the infantile and the total death-rates to an extent which even the strongest opponents of that operation had not thought possible. There are four solid lines on the diagram showing respectively, in five-year averages from 1838-42 to 1890-95, (1) the total death-rate per 1,000 living, (2) the infant death-rate under five years, (3) the same under one year, and (4), lowest of all, the small-pox death-rate under five years. The dotted line shows the percentage of total vaccinations to births. The first thing to be noted is the remarkable simultaneous rise of all four death-rates to a maximum in 1868-72, at the same that the vaccination rate attained its maximum. The decline in the death-rates from 1852 to 1860 was due to sanitary improvements which had then commenced; but the rigid enforcement of vaccination checked the decline owing to its producing a great increase of mortality in children, an increase which ceased as soon as vaccination diminished. This clearly shows that the deaths which have only recently been acknowledged as due to vaccination, directly or indirectly, are really so numerous as largely to affect the total death-rate; but they were formerly wholly concealed, and still are partially concealed, by being registered under such headings as erysipelas, syphilis, diarrhœa, bronchitis, convulsions, or other proximate cause of death. Here, then, we have indications of a very terrible fact, the deaths by various painful and often lingering diseases of thousands of children as the result of that useless and dangerous operation termed vaccination. [[p. 57]] It is difficult to explain the coincidences exhibited by this diagram in any other way, and it is strikingly corroborated by a diagram of infant mortality in London and in England which I laid before the Royal Commission, and which I here reproduce (No. X.). The early part of this diagram is from a table calculated by Dr. Farr from all the materials available in the Bills of Mortality, and it shows for each twenty years the marvellous diminution in infant mortality during the hundred years from 1730 to 1830, proving that there was some continuous beneficial change in the conditions of life. The materials for a continuation of the diagram are not given by the Registrar-General in the case of London, and I have had to calculate them for England. But from 1840 to 1890 we find a very slight fall, both in the death-rate under five years and under one year for England, and under one year for London, although both are still far too high, as indicated by the fact that in St. Saviour’s it is 213, and in Hampstead only 123 per 1,000 births. There appear to have been some causes which checked the diminution in London after 1840, then produced an actual rise from 1860 to 1870, followed by a slight but continuous fall since. The check to the diminution of the infant death-rate is sufficiently accounted for by that extremely rapid growth of London by immigration which followed the introduction of railways and which would appreciably increase the child-population (by immigration of families) in proportion to the births. The rise from 1860 to 1870 exactly corresponds to the rise in Leicester, and to the strict enforcement of infant vaccination, which was continuously high during this period; while the steady fall since corresponds also to that continuous fall in the vaccination rate due to a growing conviction of its uselessness and its danger. These facts strongly support the contention that vaccination, instead of saving thousands of infant lives, as has been claimed, really destroys them by thousands, entirely neutralising that great reduction which was in progress from [[p. 58]] the last century, and which the general improvement in health would certainly have favoured. It may be admitted that the increasing employment of women in factories is also a contributory cause of infant mortality, but there is no proof that a less proportion of women have been thus employed during the last twenty years, while it is certain that there has been a great diminution of vaccination, which is now admitted to be a vera causa of infant mortality. Before leaving the case of Leicester it will be instructive to compare it with some other towns of which statistics are available. And first as to the great epidemic of 1871-2 in Leicester and in Birmingham. Both towns were then well vaccinated, and both suffered severely by the epidemic. Thus: S.P. cases per 10,000 population . . . . . 327 (Leicester) . . . . . 213 (Birmingham) But since then Leicester has rejected vaccination to such an extent that in 1894 it had only seven vaccinations to ten thousand population, while Birmingham had 240, or more than thirty times as much, and the proportion of its inhabitants who have been vaccinated is probably less than half those of Birmingham. The Commissioners themselves state that the disease was brought into the town of Leicester on twelve separate occasions during the recent epidemic, yet the following is the result: 1891-4 S.P. cases per 10,000 population . . . . . 19 (Leicester) . . . . . 63 (Birmingham) Here we see that Leicester had less than one-third the cases of small-pox, and less than one-fourth the deaths in proportion to population than well-vaccinated Birmingham; so that both the alleged protection from attacks of the disease, and mitigation of its severity when it does attack, are shown, not only to be absolutely untrue, but to apply really, in this case, to the absence of vaccination! [[p. 59]] But we have yet another example of an extremely well-vaccinated town in this epidemic–Warrington, an official report on which has just been issued. It is stated that 99.2 per cent. of the population had been vaccinated, yet the comparison with unvaccinated Leicester stands as follows: Epidemic of 1892-3 S.P. cases per 10,000 population . . . 19.3 (Leicester) . . . 123.3 (Warrington) Here then we see that in the thoroughly vaccinated town the cases are more than six times, and the deaths more than eight times, that of the almost unvaccinated town, again proving that the most efficient vaccination does not diminish the number of attacks, and does not mitigate the severity of the disease, but that both these results follow from sanitation and isolation. Now let us see how the Commissioners, in their Final Report deal with the above facts, which are surely most vital to the very essence of the enquiry, and the statistics relating to which have been laid before them with a wealth of detail not equalled in any other case. Practically they ignore it altogether. Of course I am referring to the Majority Report, to which alone the Government and the unenlightened public are likely to pay any attention. Even the figures above quoted as to Leicester and Warrington are to be found only in the Report of the Minority, who also give the case of another town, Dewsbury, which has partially rejected vaccination, but not nearly to so large an extent as Leicester, and in the same epidemic it stood almost exactly between unvaccinated Leicester and well-vaccinated Warrington, thus: Leicester . . . . . had 1.1 mortality per 10,000 living Here again we see that it is the unvaccinated towns that suffer least, not the most vaccinated. The public of course have been terrorised by the case of Gloucester, [[p. 60]] where a large default in vaccination was followed by a very severe epidemic of small-pox. The Majority Report refers to this in par. 373, intending to hold it up as a warning, but strangely enough in so important a document, say the reverse of what they mean to say, giving to it “very little,” instead of “very much” small-pox. This case, however, has really nothing whatever to do with the question at issue, because, although anti-vaccinators maintain that vaccination has not the least effect in preventing or mitigating small-pox, they do not maintain that the absence of vaccination prevents it. What they urge is, that sanitation and isolation are the effective and only preventives, and it was because Leicester attended thoroughly to these matters, and Gloucester wholly neglected them that the one suffered so little and the other so much in the recent epidemic. On this subject every enquirer should read the summary of the facts given in the Minority Report, paragraph 261. To return to the Majority Report. Its references to Leicester are scattered over 80 pages, referring separately to the hospital staff, and the relations of vaccinated and unvaccinated to small-pox; while in only a few paragraphs (par. 480-486) do they deal with the main question and the results of the system of isolation adopted. These results they endeavour to minimise by declaring that the disease was remarkably “slight in its fatality,” yet they end by admitting that “the experience of Leicester affords cogent evidence that the vigilant and prompt application of isolation . . . is a most powerful agent in limiting the spread of small-pox.” A little further on (par. 500) they say, when discussing this very point–how far sanitation may be relied on in place of vaccination–“The experiment has never been tried.” Surely a town of 180,000 inhabitants which has neglected vaccination for twenty years, is an experiment. But a little further on we see the reason of this refusal to consider Leicester a test experiment. Par. 502 begins thus: “The question we are now discussing must, of [[p. 61]] course, be argued on the hypothesis that vaccination affords protection against small-pox.” What an amazing basis of argument for a Commission supposed to be enquiring into this very point! They then continue: “Who can possibly say that if the disease once entered a town the population of which was entirely or almost entirely unprotected, it would not spread with a rapidity of which we have in recent times had no experience?” But Leicester is such a town. Its infants–the class which always suffers in the largest numbers–are almost wholly unvaccinated, and the great majority of its adults have, according to the bulk of the medical supporters of vaccination, long outgrown the benefits, if any, of infant-vaccination. The disease has been introduced into the town twenty times before 1884, and twelve times during the last epidemic (Final Report, par. 482 and 483). The doctors have been asserting for years that once small-pox comes to Leicester it will run through the town like wild-fire. But instead of that it has been quelled with far less loss than in any of the best vaccinated towns in England. But the Commissioners ignore this actual experiment, and soar into the regions of conjecture with, “Who can possibly say?”–concluding the paragraph with–“A priori reasoning on such a question is of little or no value.” Very true. But a posteriori reasoning, from the cases of Leicester, Birmingham, Warrington, Dewsbury, and Gloucester, is of value; but it is of value as showing the utter uselessness of vaccination, and it is therefore, perhaps, wise for the professional upholders of vaccination to ignore it. But surely it is not wise for a presumably impartial Commission to ignore it as it is ignored in this Report.14 [[p. 62]] THE ARMY AND NAVY AS A CONCLUSIVE TEST In the Report of the Medical Officer of the Local Government Board for 1884, it is alleged that when an adult is revaccinated “he will receive the full measure of protection that vaccination is capable of giving him.” In the same year the Medical Officer of the General Post Office stated in a circular, “It is desirable, in order to obtain full security, that the operation (vaccination) should be repeated at a later period of life”; and the circular of the National Health Society already referred to states that “soldiers who have been revaccinated can live in cities intensely affected by small-pox without themselves suffering to any appreciable degree from the disease.” Let us then see how far these official statements are true or false. In their Final Report the Commissioners give the statistics of small-pox mortality in the Army and Navy from 1860 to 1894, and, although the latest order for the vaccination of the whole force in the Navy was only made in 1871, there can be no doubt that, practically, the whole of the men had been revaccinated long before that period;15 but certainly since 1873 all without exception, both English and foreign, were revaccinated; and in the Army every recruit has been revaccinated since 1860 (see 2nd Report, Q. 3,453, 3,455; and for the Navy, Q. 2,645, 6, 3,212-13, and 3,226-3,229). Brigade-Surgeon William Nash, M.D., informed the Commission that the vaccination and [[p. 63]] revaccination of the Army was “as perfect as endeavours can make it,” and that he can make no suggestion to increase its thoroughness (Q. 3,559, 3,560). Turning now to the diagram (No. XI.) which represents the official statistics, the two lower solid lines show the small-pox death-rate per 100,000 of the force of the Army and Navy for each year, from 1860 to 1894. The lower thick line shows the Army mortality, the thin line that of the Navy. The two higher lines show the total death-rate from disease of the Navy, and of the Home force of the Army, as the tables supplied do not separate the deaths by disease of that portion of the Army stationed abroad. Looking first at these upper lines, we notice two interesting facts. The first is, the large and steady improvement of both forces as regards health-conditions during the thirty-five years; and the second is the considerable and constant difference in the disease mortality of the two services, the soldiers having thoroughout the whole period a much higher mortality than the sailors. The decrease of the general mortality is clearly due to the great improvements that have been effected in diet, in ventilation, and in general health-conditions; while the difference in health between the two forces is almost certainly due to two causes, the most important being that the sailors spend the greater part of every day in the open-air, and in air of the maximum purity and health-giving properties, that of the open sea; while soldiers live mostly in camps or barracks, often in the vicinity of large towns, and in a more or less impure atmosphere. The other difference is that soldiers are constantly subject to temptations and resulting disease, from which sailors while afloat are wholly free. Turning now to the lower lines, we see that, as regards small-pox mortality, the Navy suffered most down to 1880, but that since that period the Army has had rather the higher mortality. This has been held to be due to the less perfect vaccination of the Navy in the earlier period, but of that there is no proof, while [[p. 64]] there is evidence as to the causes of the improvement in general health. Staff-Surgeon T. J. Preston, R.N., stated them thus: “Shorter sea-voyages; greater care not to overcrowd; plentiful and frequent supplies of fresh food; the introduction of condensed water; and the care that is now taken in the general economy and hygiene of the vessels” (Q. 3,253). These seem sufficient to have produced also the comparative improvement in small-pox mortality, especially as the shorter voyages would enable the patients to be soon isolated on shore. The question we now have to consider is, whether the amount of small-pox here shown to exist in both Army and Navy demonstrates the “full security” that revaccination is alleged to give; whether as a matter of fact our soldiers and sailors, when exposed to the contagion of intense small-pox, do suffer to “any appreciable degree”; and lastly, whether they show any immunity whatever when compared with similar populations who have been either very partially or not at all revaccinated. It is not easy to find a fairly comparable population but after due consideration it seems to me that Ireland will be the best available, as the statistics are given in the Commissioners’ Reports, and it can hardly be contended that it has any special advantages over our soldiers and sailors,–rather the other way. I have therefore given a diagram, XII., in which a dotted line shows the small-pox mortality of the Irish people of the ages 15 to 45 in comparison with the Army and the Navy mortality for the same years. (The figures for this diagram, as regards Ireland, have been calculated from the table at p. 37 of the Final Report, corrected for the ages 15 to 45 by means of Table J. at p. 274 of the Second Report.) This dotted line shows us that, with the exception of the great epidemic of 1871, when for the bulk of the Irish patients there was neither isolation nor proper treatment, the small-pox mortality of the Irish population of similar ages has been on the average below that of either the Army or the Navy; while if we take [[p. 65]] the mean mortality of the three for the same period (1864-1894) inclusive, the result is as follows: Army, mean of the annual small-pox death rate, 58 per million. If we combine the Army and Navy death-rates in the proportion of their mean strength so as to get the true average of the two forces, the death-rate is 64.3 per million, or almost exactly the same as that of Ireland. Now if there were no other evidence which gave similar results, this great test case of large populations compared over a long series of years, is alone almost conclusive; and we ask with amazement,–Why did not the Commissioners make some such comparison as this, and not allow the public to be deceived by the grossly misleading statements of the medical witnesses and official apologists for a huge imposture? For here we have on one side a population which the official witnesses declare to be as well vaccinated and revaccinated as it is possible to make it, and which has all the protection that can be given by vaccination. It is a population which, we are officially assured, can live in the midst of the contagion of severe small-pox and not suffer from the disease “in any appreciable degree.” And on comparing this population of over 200,000 men, thus thoroughly protected and medically cared for, with the poorest and least cared for portion of our country–a portion which the official witness [[p. 66]] regarding it declared to be badly vaccinated, while no amount of revaccination was even referred to–we find the less vaccinated and less cared for community to have actually a much lower small-pox mortality than the Navy, and the same as that of the two forces combined. The only possible objections that can be taken, or that were suggested during the examination of the witnesses are, that during the early portion of the period, the Navy was not wholly and absolutely revaccinated; and secondly, that troops abroad, and especially in India and Egypt, are more frequently subjected to infection. As to the first objection, even if revaccination were not absolutely universal in the Navy prior to 1873, it was certainly very largely practised, and should have produced a great difference when compared with Ireland. And the second objection is simply childish. For what are vaccination and revaccination for, except to protect from infection? And under exposure to the most intense infection they have been officially declared “not appreciably to suffer”! But let us make one more comparison comprising the period since the great epidemic of 1871-2, during which the Navy as well as the Army are admitted to have been completely revaccinated, both English and foreign. We will compare this (supposed) completely protected force with Leicester, an English manufacturing town of nearly the same population, by no means especially healthy, and which has so neglected vaccination that it may now claim to be the least vaccinated town in the kingdom. The average annual small-pox death-rate of this town for the twenty-two years 1873-94 inclusive is thirteen per million (see 4th Report, p. 440); but in order to compare with our Army and Navy we must add one-ninth for the mortality at ages 15-45 as compared with total mortality, according to the table at p. 155 of the Final Report, bringing it to 14.4 per million, when the comparison will stand as follows: [[p. 67]] Army (1873-94) small-pox death rate . . . . . 37 per million.17 It is thus completely demonstrated that all the statements by which the public has been gulled for so many years, as to the almost complete immunity of the revaccinated Army and Navy, are absolutely false. It is all what Americans call “bluff.” There is no immunity. They have no protection. When exposed to infection, they do suffer just as much as other populations, or even more. In the whole of the nineteen years 1878-1896 inclusive, unvaccinated Leicester had so few small-pox deaths that the Registrar-General represents the average by the decimal 0.01 per thousand population, equal to ten per million, while for the twelve years 1878-1889 there was less than one death per annum! Here we have real immunity, real protection; and it is obtained by attending to sanitation and isolation, coupled with the almost total neglect of vaccination. Neither Army nor Navy can show any such results as this. In the whole twenty-nine years tabulated in the Second Report the Army had not one year without a small-pox death, while the Navy never had more than three consecutive years without a death, and only six years in the whole period. Now if ever there exists such a thing as a crucial test, this of the Army and Navy, as compared with Ireland, and especially with Leicester, affords such a test. The populations concerned are hundreds of thousands; the time extends to a generation; the [[p. 68]]statistical facts are clear and indisputable; while the case of the Army has been falsely alleged again and again to afford indisputable proof of the value of vaccination when performed on adults. It is important, therefore, to see how the Commissioners deal with these conclusive test-cases. They were appointed to discover the truth and to enlighten the public and the legislature, not merely to bring together huge masses of undigested facts. What they do is, to make no comparison whatever with any other fairly comparable populations, to show no perception of the crucial test they have to deal with, but to give the Army and Navy statistics separately, and as regards the Army piecemeal, and to make a few incredibly weak and unenlightening remarks. Thus, in par. 333, they say that, during the later years, as the whole force became more completely revaccinated, small-pox mortality declined. But they knew well that during the same period it declined over all England, Scotland, and Ireland, with no special revaccination, and most of all in unvaccinated Leicester! Then with regard to the heavy small-pox mortality of the wholly revaccinated and protected troops in Egypt, they say, “We are not aware what is the explanation of this.” And this is absolutely all they say about it! But they give a long paragraph to the Post Office officials, and make a great deal of their alleged immunity. But in this case the numbers are smaller, the periods are less, and no statistics whatever are furnished except for the last four years! All the rest is an extract from a parliamentary speech by Sir Charles Dilke in 1883, stating some facts, furnished of course by the medical officers of the Post Office, and therefore not to be accepted as evidence.18 This slurring over the damning evidence of the [[p. 69]] absolute inutility of the most thorough vaccination possible, afforded by the Army and Navy, is sufficient of itself to condemn the whole Final Report of the majority of the Commissioners. It proves that they were either unable or unwilling to analyse carefully the vast mass of evidence brought before them, to separate mere beliefs and opinions from facts, and to discriminate between the statistics which represented those great “masses of national experience” to which Sir John Simon himself has appealed for a final verdict, and those of a more partial kind, which may be vitiated by the prepossessions of those who registered the facts. That they have not done this, but without any careful examination or comparison have declared that revaccinated communities have “exceptional advantages” which, as a matter of fact, the Report itself show they have not, utterly discredits all their conclusions, and renders this Final Report not only valueless but misleading. [[p. 70]] CHAPTER V CRITICAL REMARKS ON THE “FINAL REPORT” Before proceeding to sum up the broad statistical case against vaccination, it may be well here to point out some of the misconceptions, erroneous statements, vague opinions, and conclusions which are opposed to the evidence, which abound in this feeble Report. And first, we have the repetition of an oft-corrected and obviously erroneous statement as to the absolute identity of the vaccinated and the unvaccinated, except on the one point of vaccination. The Commissioners say: “Those, therefore, who are selected as being vaccinated persons might just as well be so many persons chosen at random out of the total number attacked. So far as any connection with the incidence of, or the mortality from, small-pox is concerned, the choice of persons might as well have been made according to the colour of the clothes they wore (Final Report, par. 213). But there are tables in the Reports showing that about one-seventh of all small-pox deaths occur in the first six months of life, and by far the larger part of this mortality occurs in the first three months. The age of vaccination varies actually from three to twelve months, and many children have their vaccination specially delayed on account of ill-health, so that the “unvaccinated” always include a large proportion of those who, merely because they are infants, supply a much larger proportion of deaths [[p. 71]] from small-pox than at any other age. Yet the Commissioners say the unvaccinated might as well be chosen at random, or by the colour of their clothes so far as any liability to small-pox is concerned. One stands amazed at the hardihood of a responsible body of presumably sensible and truth-seeking men who can deliberately record as a fact what is so obviously untrue. Hardly less important is it that the bulk of the unvaccinated, those who escape the vaccination officers, are the very poor, and the nomad population of the country–tramps, beggars and criminals, the occupants of the tenement houses and slums of our great cities, who, being all weekly tenants, are continually changing their residence. Such were referred to, in the Report of the Local Government Board for 1882 (p. 309), as constituting the bulk of the thirty-five thousand of default, under the heading–“Removed, not to be traced, or otherwise accounted for.” One of the Commission’s official witnesses, Dr. MacCabe, Medical Commissioner for Ireland, distinctly affirms this. He says (2nd Report, Q. 3,073) that he formerly had charge of the Dublin district, and that “out of a population of a quarter of a million, 100,000 live in tenement-houses, that is to say, houses that are let out in single rooms for the accommodation of a family. It is amongst that class, to a very great extent, that the defaulters exist. The relieving officer, when he goes to the tenement-dwelling where the birth occurred, finds that the parents have gone to some other tenement-dwelling and there is no trace of them . . . A great number of these defaulters occur in this way.” Now weekly tenants do not live in the best and most sanitary parts of towns, and the records of every epidemic show that such insanitary districts have an enormously greater proportion of the small-pox deaths than the healthier districts. Yet the Commissioners declare that there is “absolutely no difference between the vaccinated and the unvaccinated” except in [[p. 72]] respect of vaccination. Again we stand amazed at a statement so contrary to the fact. But the Commissioners must of course have believed it to be true, or they would not put it in their Final Report, upon which legislation may be founded affecting the liberties and the lives of their fellow countrymen. I submit to my readers with confidence that this statement, so directly opposed to the clearest and simplest facts and to the evidence of official witnesses, proves the incapacity of the Commissioners for the important inquiry they have undertaken. By their treatment of this part of the subject they exhibit themselves as either ignorant or careless, in either case as thoroughly incompetent. The next passage that calls for special notice here is par. 342, where they say, “We find that particular classes within the community, amongst whom revaccination has prevailed to an exceptional degree, have exhibited a position of quite exceptional advantage in relation to small-pox, although these classes have in many cases been subject to exceptional risk of contagion.” It seems almost incredible that such a statement as this could be made as a conclusion from the official evidence before the Commissioners, and it can only be explained by the fact that they never made the simplest and most obvious comparisons, and that they laid more stress on bad statistics than on good ones. They trust, for example, to the cases of nurses in hospitals,19 as to which there are absolutely no [[p. 73]] statistics in the proper sense of the term, only verbal statements by various medical men, and they overlook or forget the largest and only trustworthy body of statistics existing as to revaccination–that of the Army and Navy! “A position of quite exceptional advantage!!” When the small-pox mortality of more than 200,000 men, all revaccinated to the completest extent possible by the medical officials, shows no advantage whatever over the whole comparable population of Ireland, and a quite exceptional disadvantage in comparison with almost unvaccinated Leicester!20 There is [[p. 74]] only one charitable explanation of such a “finding” as this–namely, that the Commissioners were by education and experience wholly incompetent to deal intelligently with those great masses of national statistics which alone can furnish conclusive evidence on this question. At the end of the main inquiry, as to the effect of vaccination on small-pox (pp. 98, 99) the Commissioners adopt a very hesitating tone. They say that–“where vaccination has been most thorough the protection appears to have been greatest,” and that “the revaccination of adults appears to place them in so favourable a condition as compared with the unvaccinated.” But why say “appears” in both these cases? It is a question of fact, founded on ample statistics, which show us clearly and unmistakably–as in comparing Leicester with other towns–that vaccination gives no protection whatever, and that the best and most thorough revaccination, as in the Army and Navy, does not protect at all! It is no question of “appearing” to protect. As a fact, it does not protect, and does not appear to do so. The only explanation of the use of this word “appears” is that the Commissioners have founded their conclusions, not upon the statistical evidence at all, but upon the impressions and beliefs of the various medical officials they examined, who almost all assumed the protection as an already established fact. Such was the case of the army-surgeon who declared that the deaths were much fewer than they would have been without revaccination; and who, on being asked why he believed so, answered that it was from reading of the [[p. 75]] small-pox mortality in pre-vaccination times! He had made no comparisons, and had no figures to adduce. It was his opinion, and that of the other medical officers, that it was so. And the Commissioners apparently had always held the same opinions, which, being confirmed by the opinions of other official witnesses, they concluded that comparisons of the revaccinated Army and Navy with ordinary death-rates were as unnecessary as they would certainly have been puzzling to them. Hence “appears” in place of “is” or “does”; and their seven conclusions as to the value and protectiveness of vaccination all under the heading–“We think,” not “We are convinced,” or “It has been proved to us,” or “The statistics of the Army and Navy, of Ireland, of Leicester and of many other places, demonstrate the (“protectiveness” or “inutility”–as the case may be) of vaccination.” I trust that I have now convinced my readers that the best evidence–the evidence to which Sir John Simon and Dr. Guy have appealed–DEMONSTRATES complete INUTILITY, as against what “appears” to the Commissioners and what they “think.” One other matter must be referred to before taking leave of the Commissioners. I have already shown how completely they ignore the elaborate and valuable evidence, statistical tables and diagrams, furnished by those who oppose vaccination, such as were brought before them by Mr. Biggs of Leicester, Mr. A. Wheeler, and Mr. William Tebb, who, though all were examined and cross-examined on the minutest details, might as well never have appeared so far as any no ice in the Final Report is concerned. But there is also a very elaborate paper contributed by Dr. Adolf Vogt, Professor of Hygiene and Sanitary Statistics in the University of Berne, who offered to come to London and submit to cross-examination upon it, which, however, the Commission did not consider necessary. This paper, a translation of which is printed in the Appendix to the 6th Report, p. 689, is especially valuable as the work of a thorough statistician, who, from [[p. 76]] his position, has access to the whole body of European official statistics, and his discussion goes to the very root of the whole question. The treatise is divided into nine chapters, and occupies thirty-four closely printed pages of the Blue Book; but, being an elaborate argument founded mainly on a scientific treatment of statistics, there was probably no member of the Commission capable of adequately dealing with it. Yet it is of more value than fully nine-tenths of the remainder of the voluminous reports, with their 31,398 questions and answers. Professor Vogt’s treatise covers almost the whole ground, medical and statistical, and enforces many of the facts and arguments I have myself adduced. But there are two points which must be especially mentioned. His first chapter is headed– “A Previous Attack of Small-pox does not Confer Immunity.” I have long been of opinion that this was the case, and have by me a brief statement, written six years since, to show that the rarity of second attacks may in all probability be fully explained by the doctrine of chances. But I had not statistics sufficient to prove this. Professor Vogt, however, having the statistical tables of all Europe at his command, is able to show not only that the calculus of probabilities itself explains the rarity of a second attack of small-pox, but that second attacks occur more frequently than they should do on the doctrine of chances alone, indicating that, instead of there being any immunity, there is really a somewhat increasedsusceptibility to a second attack!21 This being [[p. 77]] the case, it becomes really ludicrous to read the questions and answers and the serious discussions as to whether a “good vaccination” protects more or less than a previous attack of small-pox. Some think the protection is the same, but the greater number think [[p. 78]] it is not quite so much. Even the most ardent vaccinists do not claim a greater protection. But none of them ever doubt the fact of the protection gained by having had the disease, and yet none of them, nor any of the Commissioners, thought that any evidence, much less proof, of the fact itself was needed. They took it for granted. “Everybody knows it.” “Very few people have small-pox a second time.” No doubt. But very few people suffer from any special accident twice–a shipwreck, or railway or coach accident, or a house on fire; yet one of these accidents does not confer immunity against its happening a second time. The taking it for granted that second attacks of small-pox, or of any other zymotic disease, are of that degree of rarity as to prove some immunity or protection indicates the incapacity of the medical mind for dealing with what is a purely statistical and mathematical question. Quite in accordance with this influence of small-pox in rendering the patient somewhat more liable to catch the disease during any future epidemic, is the body of evidence adduced by Professor Vogt, showing that vaccination, especially when repeated once or several times, renders the persons so vaccinated more liable to take the disease, and thus actually increases the virulence of epidemics. This has been suspected by some anti-vaccinators; but it is, I believe, now for the first time supported by a considerable body of statistics. The other important feature in Professor Vogt’s memoir is the strong support he gives to the view that small-pox mortality is really–other things being approximately equal–a function of density of population. All the evidence I have adduced goes to show this, especially the enormously high small-pox death-rate in crowded cities in approximate proportion to the amount of crowding. Professor Vogt adds some remarkable statistics illustrating this point, especially a table in which the 627 registration districts of England and Wales are grouped according to their density of population, from one district having only sixty-four persons to a square mile to six which have 20,698 per [[p. 79]] square mile, another column showing in how many of the years during the period 1859-1882 there were any small-pox deaths in the districts. The result shown is very remarkable. In the most thinly populated district no small-pox death occurred in any one of the twenty-four years; in the most densely peopled districts small-pox deaths occurred in every one of the twenty-four years. And the frequency of the occurrence of small-pox in all the intervening groups of districts followed exactly the density of the population. Taking two groups with nearly the same population, the fourth group of 107 districts, with a total population of 1,840,581, had small-pox deaths in only five or six out of the twenty-four years in any of them; while the thirteenth group of thirteen districts, with a population of 1,908,838, had small-pox deaths in twenty-three out of the twenty-four years. But the first group had a density of 160 to the square mile, and the last had 8,350 to the square mile. The Commissioners dwell upon the alleged fact that neither water-supply, nor drainage, nor contaminated food produce small-pox, and urge that what is commonly understood by sanitation has little effect upon it (par. 153). But what may be termed the fundamental principle of sanitation is the avoidance of overcrowding; and this is shown by an overwhelming body of evidence invariably to influence small-pox mortality quite irrespective of vaccination.22 Yet the remarkable contribution to the mass of evidence in the “Reports” which brings out this fact most clearly, receives no notice whatever in the Final Report. [[p. 80]] CHAPTER VI SUMMARY AND CONCLUSION As the diverse aspects of the problem which has been discussed in the preceding pages are somewhat numerous and complex, owing to the vast mass of irrelevant but confusing matter with which it has been encumbered at every step of its progress for nearly a century, a brief summary of the main points here referred to, and a statement of their bearing on the essential problem, will now be given. I have first shown the nature of the tests which seemed to the early enquirers to establish the protective influence of vaccination, and have given the facts which the two greatest living specialists on the subject–Professor Crookshank and Dr. Creighton–consider to prove the fallacy or insufficiency of all the tests which were applied. This is followed by a statement of the abundant evidence which in the first ten years of the century already showed that vaccination had no protective power (pp. 10-12). But the heads of the medical profession had accepted the operation as of proved value, and the legislature, on their recommendation, had voted its discoverer £30,000 of public money, and had besides, in 1808, endowed a National Vaccine Establishment with about £3,000 a year. Reputations and vested interests were henceforth at stake, and those who adduced evidence of the failure or the dangers of vaccination were treated as fanatics, and have been so treated by the medical and [[p. 81]] official world down to the appointment of the last Royal Commission. I next give the reasons why doctors are not the best judges of the effects, beneficial or otherwise, of vaccination, and follow this by proofs of a special capacity for mis-stating facts in reference to this question which has characterized them from the beginning of the century down to our day. The successive annual reports of the National Vaccine Establishment give figures of the deaths by small-pox in London in the eighteenth century, which go on increasing like Falstaff’s men in buckram; while in our own time the late Dr. W. B. Carpenter, Mr. Ernest Hart, the National Health Society, and the Local Government Board make statements or give figures which are absurdly and demonstrably incorrect (pp. 13-18).23 I then show the existence of so unreasoning a belief [[p. 82]] in the importance of vaccination that it leads many of those who have to deal with it officially to [[p. 83]] concealments and misstatements which are justified by the desire to “save vaccination from reproach.” Thus it happened that till 1881 no deaths were regularly recorded as due to vaccination, although an increasing number of such deaths now appear in the Registrar-General’s Reports; while a few medical men, who have personally inquired into these results of vaccination, have found a large amount of mortality directly following the operation, together with a large percentage of subsequent disease, often lasting for years or during life, which, except for such private enquiries, would have remained altogether unknown and unacknowledged (pp. 18-22). The same desire to do credit to the practice which they believe to be so important leads to such imperfect or erroneous statements as to the vaccinated or unvaccinated condition of those who die of small-pox as to render all statistics of this kind faulty and erroneous to so serious an extent that they must be altogether rejected. Whether a person dies of small-pox or of some other illness is a fact that is recorded with tolerable accuracy, because the disease, in fatal cases, is among the most easily recognised. Statistics of “small-pox mortality” may, therefore, be accepted as reliable. But whether the patient is registered as vaccinated or not vaccinated usually depends on the visibility or non-visibility of vaccination-marks, either during the illness or after death, both of which observations are liable to error, while the latter entails a risk of infection which would justifiably lead to its omission. And the admitted practice of many doctors, to give vaccination the benefit of any doubt, entirely vitiates all such statistics, except in those special cases where large bodies of adults are systematically vaccinated or revaccinated. Hence, whenever the results of these imperfect statistics are opposed to those of the official records of small-pox mortality, the former must be rejected. It is an absolute law of evidence, of statistics, and of common sense that when two kinds of evidence contradict each other, that which [[p. 84]] can be proved to be even partially incorrect or untrustworthy must be rejected. It will be found that all the evidence that seems to prove the value of vaccination is of this untrustworthy character. This conclusion is enforced by the fact that the more recent hospital statistics show that small-pox occurs among the vaccinated in about the same proportion as the vaccinated bear to the whole population; thus again indicating that the earlier figures, showing that they were proportionately five or six times as numerous, and the death-rate of the unvaccinated twice or thrice that of the average of pre-vaccination days, are altogether erroneous, and are due to the various kinds of error or misstatement which have been pointed out (pp. 25-30). Having thus cleared away some of the misconceptions and fallacies which have obscured the main question at issue, and having shown that, by official admission, the only valuable evidence consists of “large masses of national statistics,” which should have been dealt with by a commission of trained statisticians, I proceed to show, by a series of diagrams embodying the official or national statistics brought before the Commission, or to be found in the Reports of the Registrar-General, what such statistics really prove; and I ask my readers to look again at those diagrams as I refer to them. Diagram I. exhibits the most extensive body of national statistics available, showing at one view the death-rates from Small-pox, from the other chief Zymotic Diseases, and the Total Mortality, from 1760 to 1896. The first portion, from 1760 to 1836, is from the “Bills of Mortality,” which, though not complete, are admitted to be, on the whole, fairly accurate as regards the variations at different periods and between different diseases. The second part, from 1838 onwards, is from the Reports of the Registrar-General, and is more complete in giving all deaths whatever. Its lines are, therefore, as it were, on a higher level than [[p. 85]] those of the earlier period, and can only be compared with it as regards proportions of the different mortalities, not so accurately as to their total amounts. The main teaching of this diagram–a teaching which the Commissioners have altogether missed by never referring to diagrams showing comparative mortalities–is the striking correspondence in average rise and fall of the death-rates of small-pox, of zymotics, and of all diseases together. This correspondence is maintained throughout the whole of the first part, as well as through the whole of the second part, of the diagram; and it proves that small-pox obeys, and always has obeyed, the same law of subservience to general sanitary conditions as the other great groups of allied diseases and the general mortality. Looking at this most instructive diagram, we see at once the absurdity of the claim that the diminution of small-pox in the first quarter of our century was due to the partial and imperfect vaccination of that period. Equally absurd is the allegation that its stationary character from 1842 to 1872, culminating in a huge epidemic, was due to the vaccination then prevailing, though much larger than ever before, not being quite universal–an allegation completely disproved by the fact that the other zymotics as a whole, as well as the general mortality, exhibited strikingly similar decreases followed by equally marked periods of average uniformity or slight increase, to be again followed by a marked decrease. There is here no indication whatever of vaccination having produced the slightest effect on small-pox mortality. The second diagram shows that, even taking the Commission’s favourite method of comparing the zymotics separately with small-pox, all of them except measles show a similar or a greater decrease during the period of official registration, and also agree in the periods of slight increase, again proving the action of the same general causes (which I have pointed out at p. 37), and leaving no room whatever for the supposed effects of vaccination. [[p. 86]] Diagram III. shows that similar phenomena occurred in England and Wales as a whole, the other zymotics and the total deaths obeying the same laws of increase and decrease as small-pox. Comparison with diagram I. shows the much greater severity of small-pox epidemics in London, illustrating the fact, which all the statistical evidence of all countries strikingly enforces, that small-pox mortality is, other things being equal, a function of density of population, while it pays no regard whatever to vaccination. This is further shown by the short, thick dotted line which exhibits the total number of vaccinations since 1872, when private as well as public vaccinations were first officially recorded, and which proves that the continuous decrease of vaccination since 1882 has been accompanied by a decided decrease, instead of an increase, in small-pox mortality. Diagram IV. shows the statistics of mortality in Ireland and Scotland from small-pox and certain chosen zymotics, from the tables which were laid before the Commission by the official advocates of vaccination. These show two striking facts, which the Commissioners failed to notice in their Final Report. First, the smaller amount of small-pox mortality in Ireland than in Scotland, the latter being alleged to be well vaccinated, the former imperfectly so; and, secondly, the similar difference in the two chosen diseases and the general parallelism of the two. Here again we see clearly the influence of density of population, Scotland having a very much larger proportion of its inhabitants living in large manufacturing towns. The next three diagrams, V., VI., and VII., show small-pox mortality in Sweden, Prussia, and Bavaria–countries which at previous enquiries were adduced as striking examples of the value of vaccination. They all show phenomena of the same character as our own country, but far worse as regards epidemics in the capitals; that of Stockholm, in 1874, causing a death-rate more than 50 per cent. higher than [[p. 87]] during the worst epidemic of the last century in London! The diagram of small-pox and zymotics in Bavaria is given merely because the statistics were brought before the Commission as a proof of the beneficial results of vaccination in well-vaccinated communities. It was alleged by Dr. Hopkirk that almost the whole of the population were vaccinated, and admitted by him that of the 30,742 cases of small-pox in 1871 no less than 95.7 per cent. were vaccinated! The epidemic was, however, less severe than in Prussia, again showing the influence of density of population, less than one-seventh of the Bavarians inhabiting towns of over 20,000, while one-fourth inhabit similar towns in Prussia; but we see that during the latter half of the period chosen small-pox greatly increased, and the other zymotics remained very high, indicating general insanitary conditions. And this case was specially brought before the Commission as a proof of the benefits of vaccination! In their Final Report the Commissioners omit to point out that it really indicates the very reverse. We then come to the two cases that afford most conclusive tests of the absolute uselessness of vaccination–Leicester and our Army and Navy. Diagram VIII. shows the death-rates from small-pox and from the other zymotics in LEICESTER during the period of official registration, together with the percentage of vaccinations to births. Up to 1872 Leicester was a fairly well-vaccinated town, yet for thirty-four years its small-pox mortality, in periodical epidemics, remained very high, corresponding generally with the other zymotics. But immediately after the great epidemic of 1872, which was much worse than in London, the people began to reject vaccination, at first slowly, then more rapidly, till for the last eight years less than 5 per cent. of the births have been vaccinated. During the whole of the last twenty-four years small-pox deaths have been very few, and during twelve consecutive years, 1878-89, there was a total of only eleven small-pox deaths in this populous town. [[p. 88]] Diagram IX. is equally important as showing a remarkable correspondence, if not a causal relation, between vaccination and disease. From 1848 to 1862 there was a considerable decrease of both general and infant mortality, and also in infant mortality from small-pox. This, Mr. Biggs tells us, was when important sanitary improvements were in progress. Then the more thorough enforcement of vaccination set in (as shown by the dotted line), and was accompanied by an increase of all these mortalities. But so soon as the revolt against vaccination began, till the present time, when it has diminished to about 2 or 3 per cent. of births, all mortalities have steadily decreased, and that decrease has been especially marked in infant lives. It is very suggestive that the lines of infant mortality have now reached the position they would have had if the slow decrease during 1850-60 had been continued, strongly indicating that some special cause sent them up, and the removal of that cause allowed them to sink again; and during that very period vaccination increased and then steadily decreased. I venture to declare that in the whole history of vaccination there is no such clear and satisfactory proof of its having saved a single life as these Leicester statistics afford of its having been the cause of death to many hundreds of infants. Diagram X. exhibits the check to the decrease in infant mortality, both in London and for England, since the enforcement of vaccination (p. 57), and thus supports and enforces the conclusions derived from the preceding diagram. THE ARMY AND NAVY I next discuss in some detail what is undoubtedly the most complete and crucial test of the value or uselessness of vaccination to be found anywhere in the world. Since 1860 in the Army, and 1872 in the Navy, every man without exception, English or foreign, has been vaccinated on entering the service, though for long before that period practically the [[p. 89]] whole force was vaccinated or revaccinated. Diagrams XI. and XII. exhibit the result of the statistics presented to the Commission, showing for the Navy the death-rate from disease and that from small-pox for the whole force; and for the Army the death-rate from small-pox for the whole force, and that from disease for the home force only, foreign deaths from disease not being separately given. Here we note, first, as in all the other communities we have dealt with, the general correspondence between the two lines of total disease mortality and small-pox mortality, resulting from the greater attention given to sanitation and to general health conditions of both forces during the last thirty or forty years. But, instead of small-pox mortality absolutely vanishing with the complete revaccination in the Army since 1860, it shows but a small improvement as compared with general disease mortality; just as if some adverse cause were preventing the improvement. In the Navy the improvement is somewhat greater, and more nearly comparable with that of general disease mortality. There is, therefore, as regards proportionate decrease, no indication whatever of any exceptional cause favourably influencing small-pox. In diagram XII. I compare the small-pox mortality of the Army and Navy with that of Ireland from tables given in the Final Report and the Second Report; and we find that this whole country (at ages 15-45) has actually a much lower small-pox mortality than the Army, while it is a little more than in the Navy, although the mortality during the great epidemic was higher than any that affected the Army or Navy, owing to its rapid spread by infection in the towns. But the proportionate numbers dying of small-pox in a series of years is, of course, the final and absolute test; and, applying this test, we find that these revaccinated soldiers and sailors have suffered in the thirty-one years during which the materials for comparison exist, to almost exactly the same extent as poor, half-starved, imperfectly [[p. 90]] vaccinated Ireland (p. 65)! Another and still more striking comparison is given. The town of Leicester is, and has been for the last twenty years, the least vaccinated town in the kingdom. Its average population from 1873 to 1894 was about two-thirds that of the Army during the same period. Yet the small-pox deaths in the Army and Navy were thirty-seven per million, those of Leicester under fifteen per million. Thus, whether we compare the revaccinated and thoroughly “protected” Army and Navy with imperfectly vaccinated Ireland, or with almost unvaccinated Leicester, we find them either on a bare equality or worse off as regards small-pox mortality. It is not possible to have a more complete or crucial test than this is, and it absolutely demonstrates the utter uselessness, or worse than uselessness, of revaccination!24 In the face of this clear and indisputable evidence, all recorded in their own Reports, the Commissioners make the astounding statement: “We find that particular classes within the community amongst whom revaccination has prevailed to an exceptional degree have exhibited a position of quite exceptional advantage in relation to small-pox, although these classes have in many cases been subject to exceptional risk of contagion” (Final Report, p. 90, par. 342). And again: “The fact that revaccination of adults appears to place them in so favourable a condition as compared with the unvaccinated,” etc. (Final Report, p. 98, Sec. 375). What can be said of such statements as these, but simply that they are wholly untrue. And the fact that the majority of the Commissioners did not know this, because they never compared the different groups of facts in their own reports which prove them to be untrue, demonstrates at once their complete [[p. 91]] incapacity to conduct such an inquiry and the utter worthlessness of their Final Report. This is a matter upon which it is necessary to speak plainly. For refusing to allow their children’s health, or even their lives, to be endangered by the inoculation into their system of disease-produced matter, miscalled “lymph,”25 hundreds and probably thousands of English parents have been fined or imprisoned and treated as criminals, while certainly thousands of infants have been officially done to death, and other thousands injured for life. And all these horrors on account of what Dr. Creighton has well termed a “grotesque superstition,” which has never had a rational foundation either of physiological doctrine or of carefully tested observations, and is now found to be disproved by a century’s dearly bought experience. This disgrace of our much-vaunted scientific age has been throughout supported by concealment of facts telling against it, by misrepresentation, and by untruths. And now a Royal Commission, which one would have supposed would have striven to be rigidly impartial, has presented a Report which is not only weak, misleading, and inadequate, but is also palpably one-sided, in that it omits in every case to make those comparisons by which alone the true meaning can be ascertained of those “great masses of national experience” to which appeal has been made by the official advocate of vaccination par excellence–Sir John Simon. I venture to think that I have here so presented the best of these statistical facts as to satisfy my readers of the certain and absolute uselessness of vaccination as a preventive of small-pox; while these same facts render it in the highest degree probable that it has [[p. 92]]actually increased susceptibility to the disease. The teaching of the whole of the evidence is in one direction. Whether we examine the long-continued records of London mortality, or those of modern registration for England, Scotland, and Ireland; whether we consider the “control experiment” or crucial test afforded by unvaccinated Leicester, or the still more rigid test in the other direction, of the absolutely revaccinated Army and Navy, the conclusion is in every case the same: that vaccination is a gigantic delusion; that it has never saved a single life; but that it has been the cause of so much disease, so many deaths, such a vast amount of utterly needless and altogether undeserved suffering, that it will be classed by the coming generation among the greatest errors of an ignorant and prejudiced age, and its penal enforcement the foulest blot on the generally beneficent course of legislation during our century. To talk of amending such legislation is a mockery. Absolute and immediate abolition is the only rational course open to us. Every day the vaccination laws remain in force parents are being punished, infants are being killed. An Act of a single clause will repeal these vile laws; and I call upon every one of our legislators to consider their responsibilities as the guardians of the liberties of the English people, and to insist that this repeal be effected without a day’s unnecessary delay. The successive Vaccination Acts were passed by means of allegations which were wholly untrue and promises which have all been unfulfilled. They stand alone in modern legislation as a gross interference with personal liberty and the sanctity of the home; while as an attempt to cheat outraged nature and to avoid a zymotic disease without getting rid of the foul conditions that produce or propagate it, the practice of vaccination is utterly opposed to the whole teaching of sanitary science, and is one of those terrible blunders which, in their far-reaching evil consequences, are worse than the greatest of crimes. * * * [[p. 93]] INDEX A. Air, importance of pure, 42. B. Bavaria, small-pox and vaccination in, 49. C. Certificates of death, often erroneous, 18. D. Davidson, Mr., on injurious effects from vaccination, 20. E. English small-pox, 1838-1895, 40. F. Farr, Dr., on decrease of infant mortality, 57. G. Gloucester epidemic due to insanitation, 60. H. Hart, Mr. E., on small-pox at Ceara, 81. I. Infant mortality in London and England, 57. J. Jenner awarded £10,000, 9. L. Lancet on vaccination disasters, 73. M. MacCabe, Dr., on vaccination in Ireland, 43. N. National Health Society’s mis-statements, 16. [[p. 95]] P. Population, density of, affecting disease, 42. R. Revaccination, officials on the value of, 62. S. Scarlatina and diphtheria in London, 37. T. Tebb, Mr. W., on 535 cases of small-pox, after vaccination before 1810, 11. U. Unvaccinated a different class from the vaccinated, 29. V. Vaccinated and unvaccinated, how determined by doctors, 25. W. Warrington and Leicester small-pox, 59. Z. Zymotic diseases in London, 36. * * * Notes Appearing in the Original Work 1. Professor Crookshank, in his evidence before the Royal Commission (4th Report, Q. 11,729) quotes Dr. De Haën, a writer on Inoculation, as saying: “Asthma, consumption, hectic or slow fever of any kind, internal ulcers, obstructed glands, obstructions of the viscera from fevers, scrofula, scurvy, itch, eruptions, local inflammations or pains of any kind, debility, suppressed or irregular menstruation, chlorosis, jaundice, pregnancy, lues venerea, whether in the parent or transmitted to the child, and a constitution under the strong influence of mercury, prevented the operation.” There is no evidence that [[p. 8]] those who applied the so-called “variolous test” in the early days of vaccination paid any attention to this long list of ailments, many of which were very prevalent at the time, and which would, in the opinion of De Haën, and of the English writer Sanders, who quotes him, have prevented the action of the virus and thus rendered the “test” entirely fallacious. With such causes as these, added to those already discussed, it becomes less difficult to understand how it was that the alleged test was thought to prove the influence of the previous vaccination without really doing so. [[beginning on p. 7]] 2. The cases of failure of vaccination here referred to are given in Mr. William White’s Story of a Great Delusion, where fuller extracts and references will be found. [[on p. 11]] 3. These extracts from the Reports are given by Mr. White in his Story of a Great Delusion. The actual deaths from small-pox during the last century are given in the Second Report of the Royal Commission, p. 290. The above statements have been verified at the British Museum by my friend Dr. Scott Tebb, and are verbally accurate. [[on p. 14]] 4. As an example of the dreadful results of vaccination, even where special care was taken, the following case from the Sixth Report of the Royal Commission (p. 128) is worthy of earnest attention. It is the evidence of Dr. Thomas Skinner, of Liverpool: 5. See Table J, p. 201, 3rd Report, and the Minority Report of the Roy. Comm., pp. 176-7. [[on p. 28]] 6. The same view is taken even by some advocates of vaccination in Germany. In an account of the German Commission for the Consideration of the Vaccination Question in the British Medical Journal, August 29, 1885 (p. 408), we find it stated: “In the view of Dr. Koch, no other statistical material than the mortality from small-pox can be relied upon; questions as to the vaccinated or unvaccinated condition of the patient leaving too much room for error.” [[on p. 29]] 7. It is always stated that only the deaths of those persons belonging to the Church of England, or who were buried in the churchyards, are recorded in the “Bills.” This seems very improbable, because the “searchers” must have visited the house and recorded the death before the burial; and as they were of course paid a fee for each death certified by them, they would not enquire very closely as to the religious opinions of the family, or where the deceased was to be buried. A friend of mine who lived in London before the epoch of registration informs me that he remembers the “searchers'”visit on the occasion of the death of his grandmother. They were two women dressed in black; the family were strict dissenters, and the burial was at the Bunhill Fields cemetery for Nonconformists. This case proves that in all probability the “Bills” did include the deaths of many, perhaps most, Nonconformists. [[on p. 32]] 8. Final Report of Roy. Comm., p. 20 (85). [[on p. 33]] 9. As an example of the Commissioners’ statistical fallacies in treating the subject of changed age-incidence, see Mr. Alexander Paul’s A Royal Commission’s Arithmetic(King & Son, 1897), and, especially, Mr. A. Milnes’ Statistics of Small-pox and Vaccination in the Journal of the Royal Statistical Society, September, 1897. [[on p. 44]] 10. The highest small-pox mortality in London was in 1772, when 3,992 deaths were recorded in an estimated population of 727,000, or a death-rate of not quite 5,500 per million. (See Second Report, p. 290.) [[on p. 46]] 11. The small-pox deaths under one year in England have varied during the last fifty years from 8.6 to 27 per cent. of the whole. (See Final Report, p. 154.) [[on p. 49]] 12. This almost exactly agrees with the ages of the boys who are admitted between nine and eleven, and leave at fourteen. (See Low’s Handbook of London Charities.) [[on p. 51]] 13. From 1850 to 1873 the private vaccinations have been estimated according to their proportion of the whole since they have been officially recorded. [[on p. 55]] 14. Although the Commission make no mention of Mr. Bigg’s tables and diagrams showing the rise of infant-mortality with increased vaccination, and its fall as vaccination diminished, they occupied a whole day cross-examining him upon them, endeavouring by the minutest criticism to diminish their importance. Especially it was urged that the increase or decrease [[p. 62]] of mortality did not agree in detail with the increase or decrease of vaccination, forgetting that there are numerous causes contributing to all variations of death-rate, while vaccination is only alleged to be a contributory cause, clearly visible in general results, but not to be detected in smaller variations (see Fourth Report, Q. 17,513-17,744, or pp. 370 to 381). Mr. Bigg’s cross-examination in all occupies 110 pages of the Report. [[beginning on p. 61]] 15. It was introduced into the Navy in 1801, and in that year the medical officers of the fleet presented Jenner with a special gold medal! [[on p. 62]] 16. These figures (for the Army and Navy) are obtained by averaging the annual death-rates given in the tables referred to, and are therefore not strictly accurate on account of the irregularly varying strength of the forces. But the error is small. In the case of the Navy, from 1864 to 1888 the mortality accurately calculated comes out more, by nearly six per cent. than the mean above given, and in the case of the Army for the same years about one per cent. more. For Ireland the calculation has been accurately made by means of the yearly populations given at p. 37 of the Final Report, but for the Army and Navy materials for the whole period included in the diagrams materials are not available in any of the Reports. [[on p. 65]] 17. The figures for the Army are obtained from the Second Report, p. 278, down to 1888, the remaining six years being obtained from the Final Report, pp. 86, 87; but this small addition has involved a large amount of calculation, because the Commissioners have given the death-rates per 10,000 strength of four separate forces–Home, Colonial, Indian, and Egyptian, and have not given the figures for the whole Army, so as to complete the table in the Second Report. The figures for the Navy are obtained from the Final Report, p. 88. [[on p. 67]] 18. Neither Sir C. Dilke nor the Post Office medical officers of the period referred to gave evidence before the Commission, and it shows to what lengths the Commissioners would go to support vaccination when such unverified verbal statements are accepted in their Final Report. [[on p. 68]] 19. As regards the case of the nurses in small-pox hospitals, about which so much has been said, I brought before the Commission some evidence from a medical work, which sufficiently disposes of this part of the question. In Buck’s Treatise on Hygiene and the Public Health, Vol. II., we find an article by Drs. Hamilton and Emmett on “Small-pox and other Contagious Diseases,” and on page 321 thereof we read: “It is a fact fully appreciated by medical men, that persons constantly exposed to small-pox very rarely contract the disease. In the case of physicians, health-inspectors, nurses, sisters of charity, hospital orderlies, and some others, this is the rule; and of over 100 persons who have been to my [[p. 73]] knowledge constantly exposed, some of them seeing as many as 1,000 cases, I have never personally known of more than one who has contracted the disease; but there are many writers who believe perfect immunity to be extremely rare. In this connection attention may be called to the exemption of certain persons who occupy the same room, and perhaps bed, with the patients, and though sometimes never vaccinated, altogether escape infection.” 20. It is a common practice of vaccinists to quote the German Army as a striking proof of the good effects of revaccination; but as our own Army is as well vaccinated as the Army surgeons with unlimited power can make it, it is unlikely that the Germans can do so very much better. And there is some reason to think that their statistics are less reliable than our own. Lieut.-Col. A. T. Wintle, (late) R.A, has published in the Vaccination Inquirer extracts from a letter from Germany stating, on the authority of a German officer, that the Army statistics of small-pox are utterly unreliable. It is said to be the rule for Army surgeons to enter small-pox cases as skin-disease or some other “appropriate illness,” while large numbers of small-pox deaths are entered as “sent away elsewhere.” We had better therefore be content with our own Army and Navy statistics, though even here there is some concealment. In 1860 Mr. Duncombe, M.P., moved for a return of the disaster at Shorncliffe Camp, where, it was alleged, 30 recruits were vaccinated, and six died of the results, but the return was refused. A letter in the Lancet of July 7, 1860, from a “Military Surgeon” stated that numbers of soldiers have had their arms amputated in consequence of mortification after vaccination; and a Baptist minister and ex-soldier, the Rev. Frederick J. Harsant, gave evidence before the Commission of another Shorncliffe disaster [[p. 74]] in 1868, he himself, then a soldier, having never recovered, and having had unhealed sores on various parts of his body for more than 20 years. Eighteen out of the twenty men vaccinated at the same time suffered; some were months in hospital and in a much worse condition than himself (6th Report, p. 207). In the same volume is the evidence of twenty medical men, all of whom have witnessed serious effects produced by vaccination, some being of a most terrible and distressing character. [[beginning on p. 73]] 21. Brief statement of the argument: The chances of a person having small-pox a second time may be roughly estimated thus: Suppose the average annual death-rate by small-pox to be 500 per million, and the average duration of life forty years. Then the proportion of the population that die of small-pox will be 500 x 40 = 20,000 per million. If the proportion of deaths to cases is one to five, there will be 100,000 cases of small-pox per million during the life of that million, so that one-tenth of the whole population will have small-pox once during their lives. 22. It is not alleged that over-crowding, per se, is the direct cause of small-pox, or of any other zymotic disease. It is, perhaps rather a condition than a cause; but under our present social economy it is so universally associated with various causes of disease–impure air, bad drainage, bad water supply, unhealthy situations, unwholesome food, overwork, and filth of every description in houses, clothing, and persons–that it affords the most general and convenient indication of an unhealthy as opposed to a healthy mode of life, and, while especially applying to zymotic diseases, is also so generally prejudicial to health as to produce a constant and very large effect upon the total mortality. [[on p. 79]] 23. To the cases I have already given I may now add two others, because they illustrate the recklessness in making assertions in favour of vaccination which scorns the slightest attempt at verification. In the first edition of Mr. Ernest Hart’s Truth about Vaccination (p. 4), it is stated, on the authority of a member of Parliament recently returned from Brazil, that during an epidemic of small-pox at the town of Ceara in 1878 and 1879, out of a population not exceeding 70,000 persons there were 40,000 deaths from small-pox. This was repeated by Dr. Carpenter during a debate in London, in February, 1882, and only when its accuracy was called in question was it ascertained that at the time referred to the population of Ceara was only about 20,000, yet the M.P. had stated–with detailed circumstance–that “in one cemetery, from August 1878, to June 1879 27,064 persons who had died of small-pox had been buried.” Gazetteers are not very recondite works, and it would have been not difficult to test some portion of this monstrous statement before printing it. Jenner’s biographer tells us that he had a horror of arithmetical calculations, due to a natural incapacity, which quality appears to be a special characteristic of those who advocate vaccination, as the examples I have given sufficiently prove. 24. So late as 1892 (Jan. 16) the Lancet declared in a leading article: “No one need die of small-pox; indeed, no one need have it unless he likes–that is to say, he can be absolutely protected by vaccination once repeated.” Surely, never before was misstatement so ignorantly promulgated, or so completely refuted! [[on p. 90]] 25. “LYMPH, a colourless nutritive fluid in animal bodies” (Chambers’ Dictionary). How misleading to apply this term to a product of disease, used to produce another disease, and now admitted to be capable of transmitting some of the most horrible diseases which afflict mankind–syphilis and leprosy! [[on p. 91]] * * * [[THE DIAGRAMS]] DIAGRAM I. London Death-rates per Million Living from 1760 to 1896.
The Upper line shows rates of Death from All Causes. The Middle line shows rates of Death from Zymotic Diseases, including Measles, Fevers, Whooping-cough, and Diphtheria. The Lower line (shaded for distinctness), Small-pox.
DIAGRAM II. Showing Death-rates from the Chief Zymotic Diseases in London from 1838 to 1896.
From the Registrar-General’s Annual Summary, 1896, Table 14, page xxxiii., and 1888, Table 12, for first nine years. These diagrams show the same facts as Dr. Whitelegge’s Diagram E. in the Sixth Report of the Royal Commission, page 660, but in a simpler form.
DIAGRAM III. Small-pox, Vaccinations, Zymotics, and Total Death-rate in England and Wales.
Small-pox from Final Report, Tab. B. p. 155, and Registrar-General’s Report, 1895, Table 24. Vaccinations from Final Report, p. 34. Zymotic diseases from Registrar-General’s Report (1895), Table 24, Columns 3 to 9. Total Death-rate from Registrar-General’s Report, 1895, Table 3.
DIAGRAM IV. Comparison of Scotland and Ireland as regards their Death-rates from Small-pox and two Zymotics (Measles and Scarlet-fever).
From Tables given in the Roy. Comm. Final Report. (See pages 35, 37, 42, and 44.)
DIAGRAM V. Sweden. Small-pox and Total Death-rates, and Stockholm Small-pox Epidemics.
These death-rates have been calculated by myself from the official tables of Small-pox and total deaths, and populations in the Sixth Report, pages 752-3.
Small-pox death-rates in Prussia __________ Epidemics in Berlin – – – – – – – – –
DIAGRAM VII. Bavaria. Mortality from Small-Pox and other Zymotic Diseases in the years 1858-73.
From Tables in the Second Report, pp. 337-8.
DIAGRAM VIII. Showing the Death-rates per Million living by Small-pox and Zymotic Diseases, from 1838 to 1896, in Leicester.
The dotted line shows the percentage of Vaccinations to Births. N.B.–Before 1862 private vaccinations have been estimated.
DIAGRAM IX. This Diagram shows various Death-rates in Leicester, in five-year Averages.
The dotted line shows the percentage of vaccinations to total births.
The upper portion of this diagram shows the Infant Mortality of London from 1730 to 1830, from Dr. Farr’s tables in McCulloch’s Statistical Account of the British Empire, vol. ii., p. 543 (1847). From 1840 to 1890 shows the Infant Mortality of England calculated from the Reports of the Registrar-General (see 3rd Report, p. 197, Table O). Materials for the continuation of Dr. Farr’s London Table (under 5 years) are not given by the Registrar-General.
Lower Thick line shows the Small-pox mortality per 100,000 in the Army. Upper Thick line shows the total Disease Mortality in the Army (Home Force). The two Thin lines show the corresponding Mortalities in the Navy.
DIAGRAM XII. Small-pox Mortality per 100,000. The Army and Navy as compared with Ireland.
From the earliest year given for Ireland in the Reports of the Royal Commission. * * * * * |
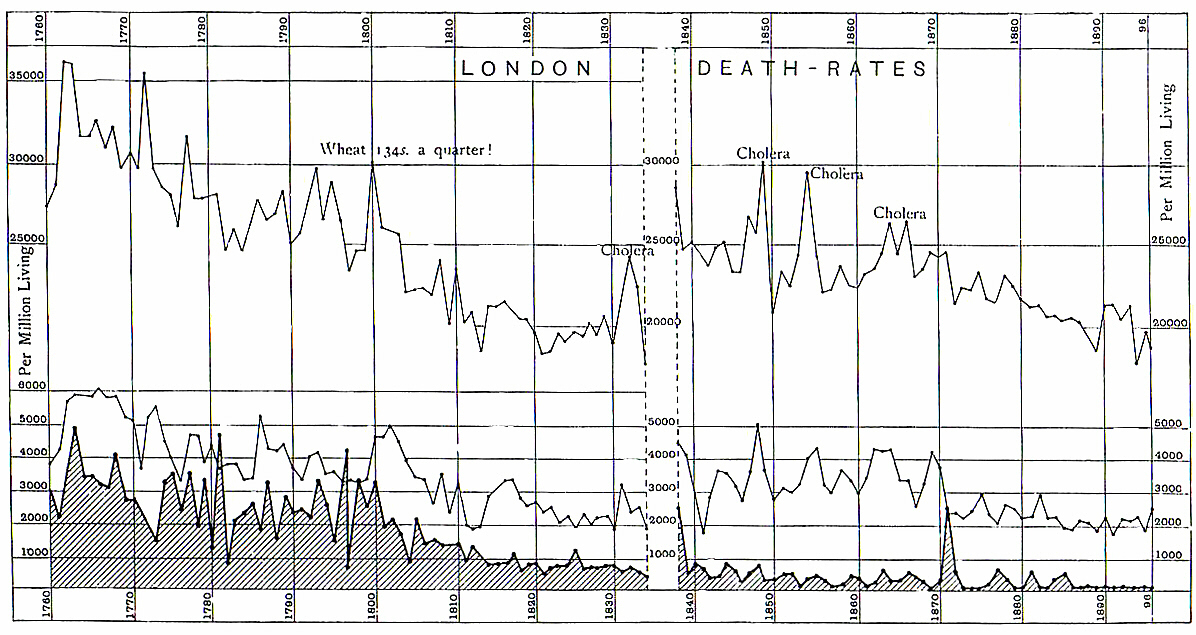
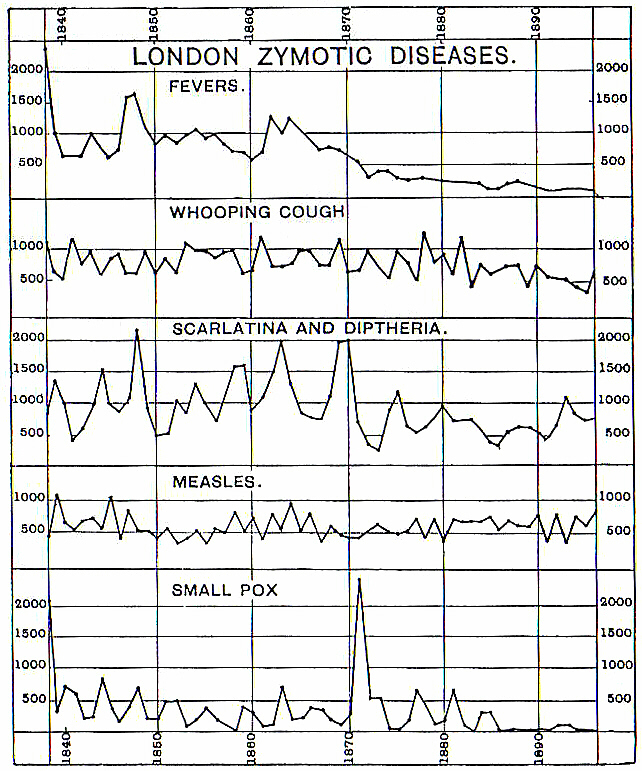
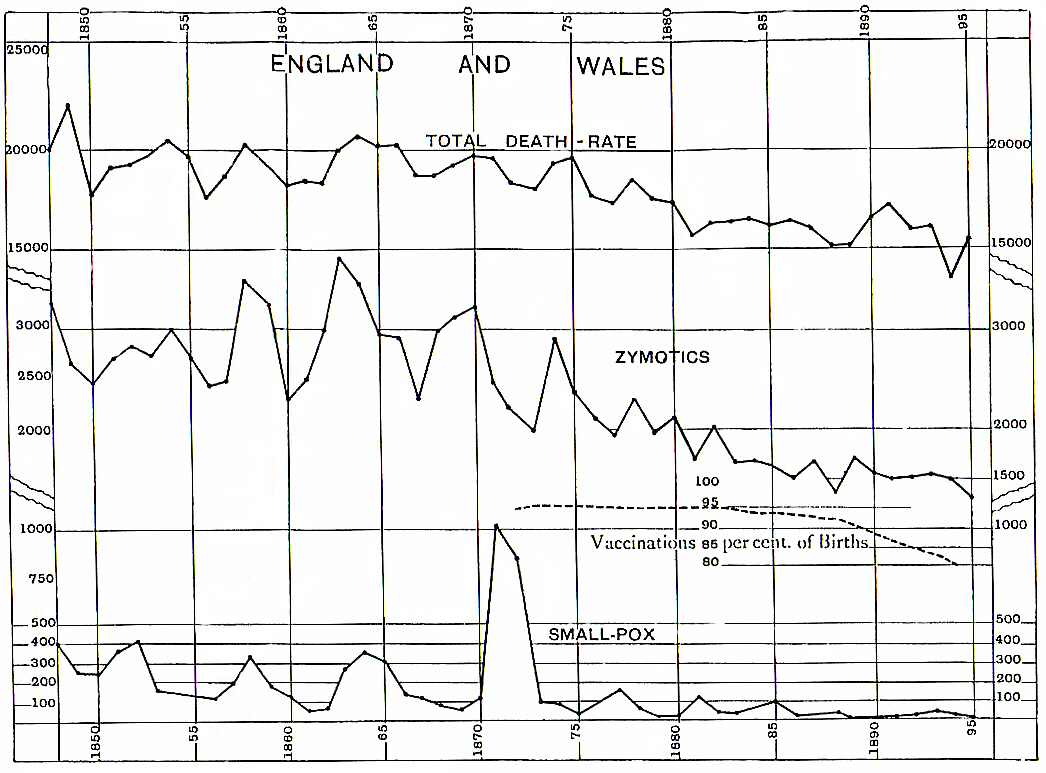
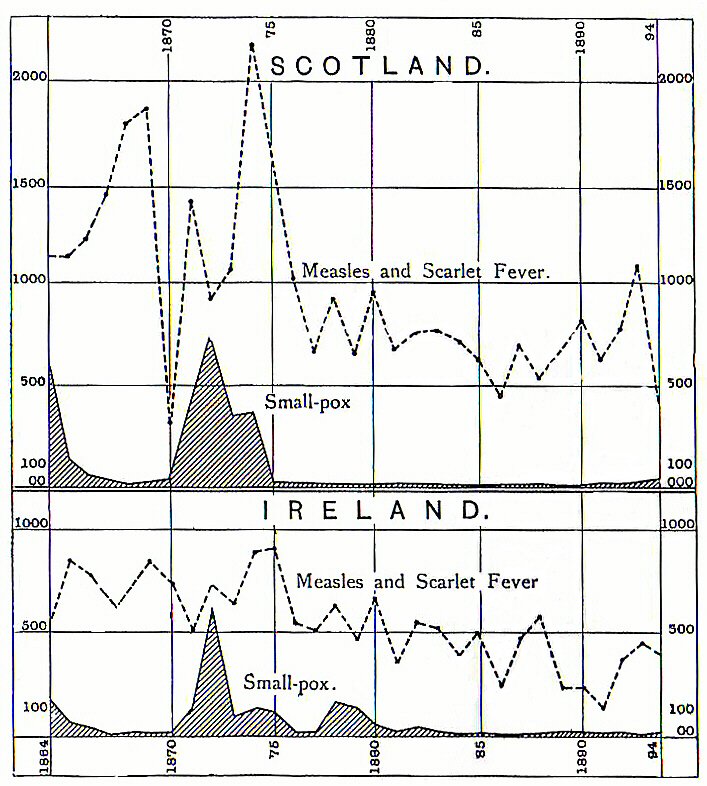
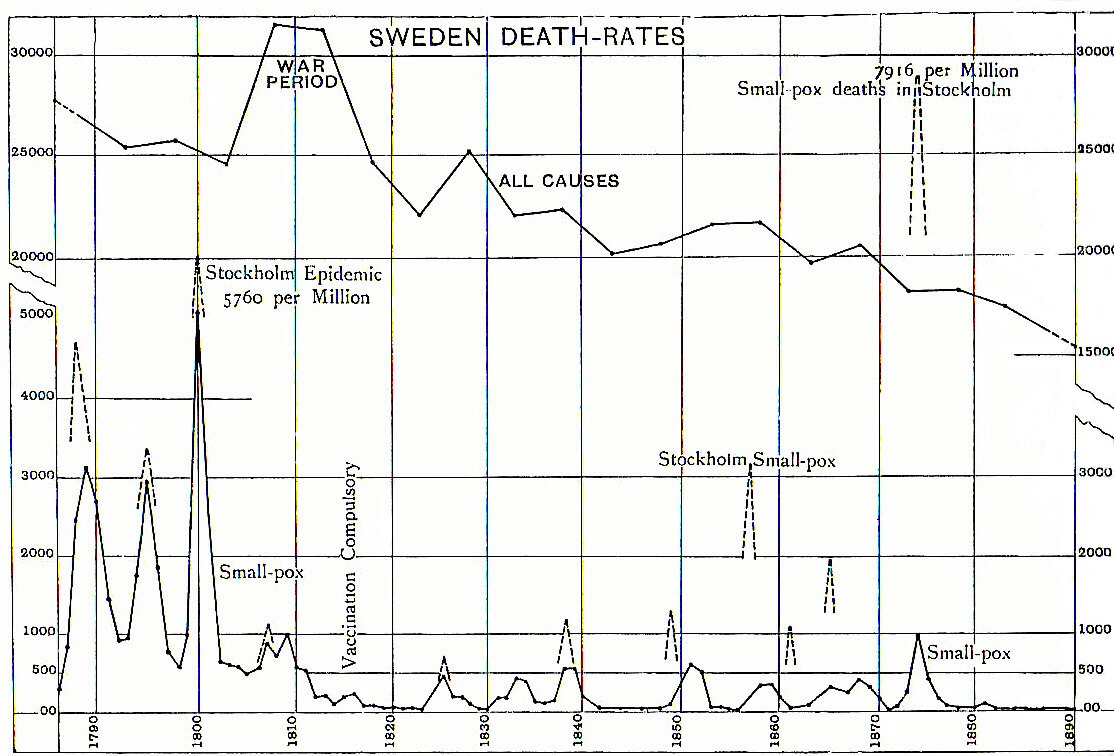
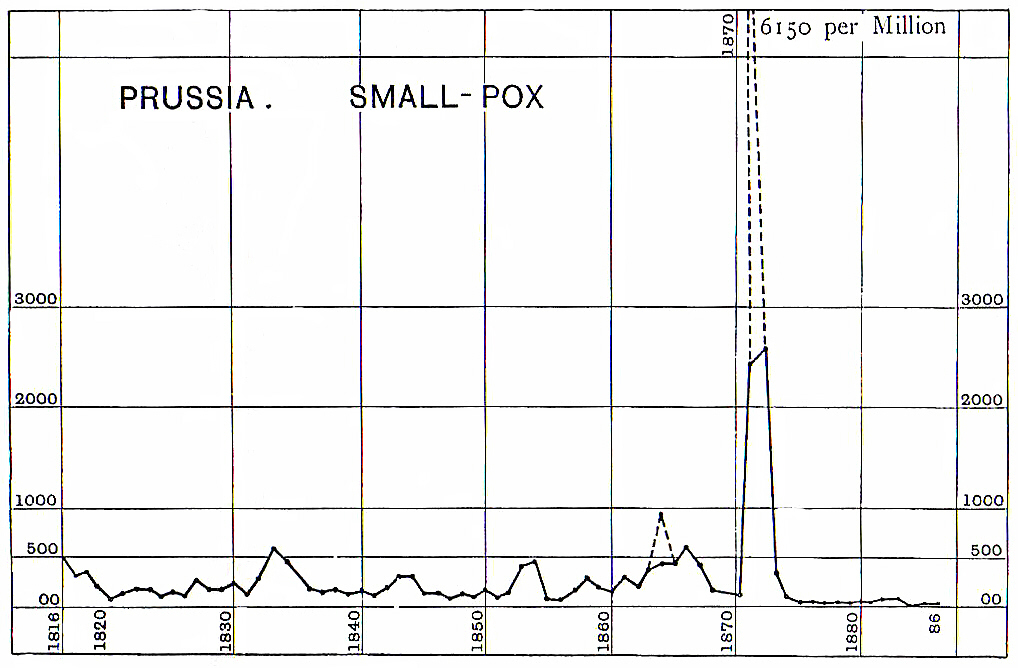
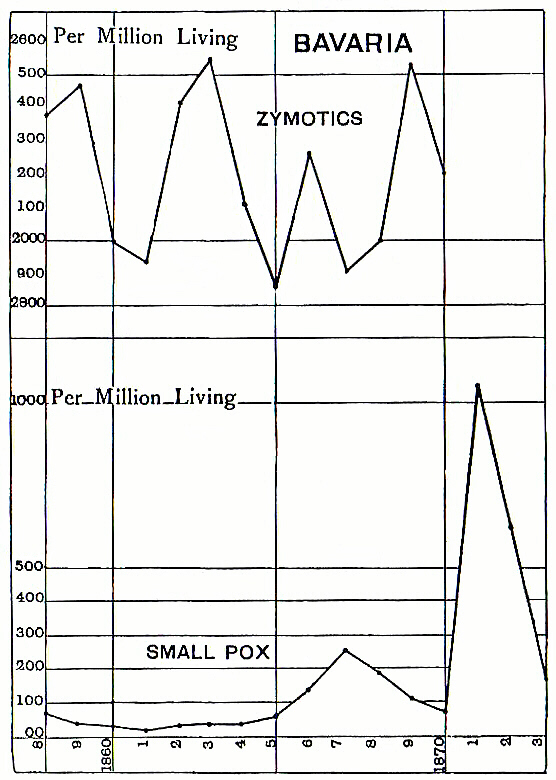
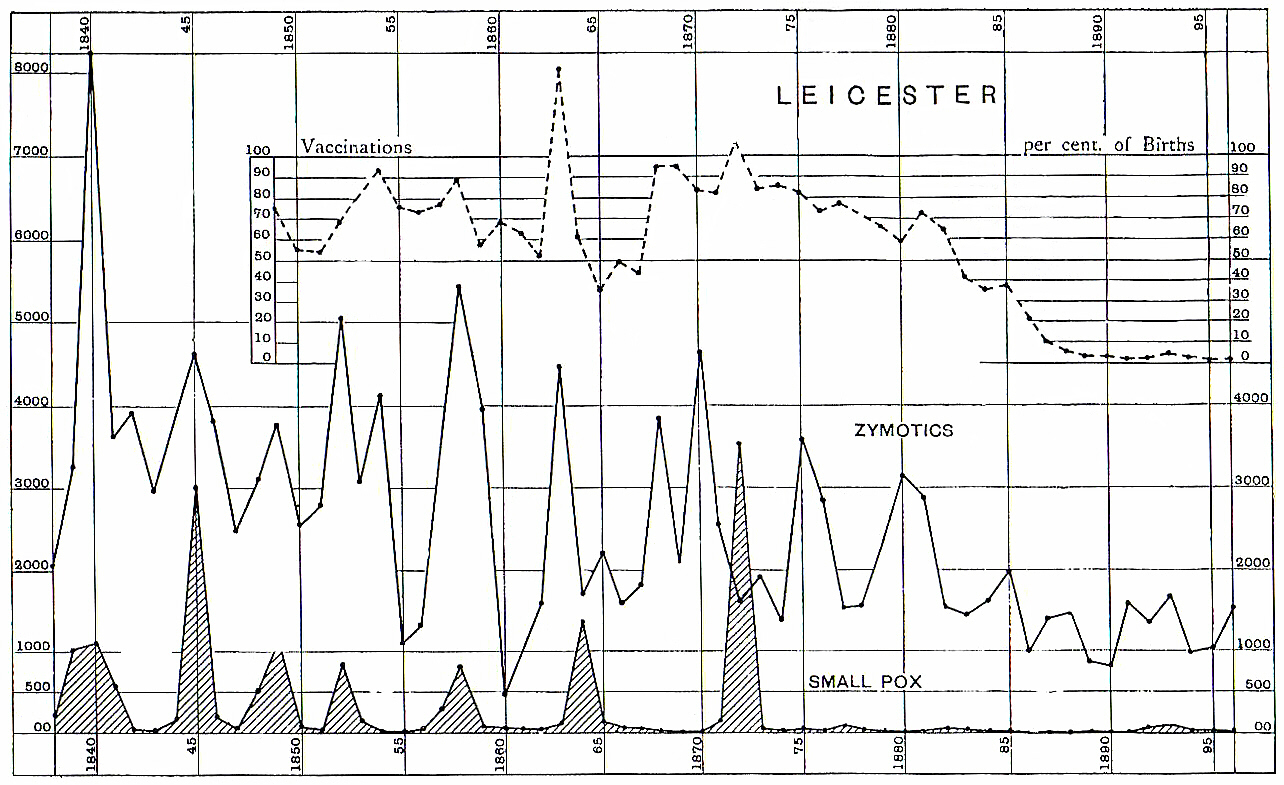
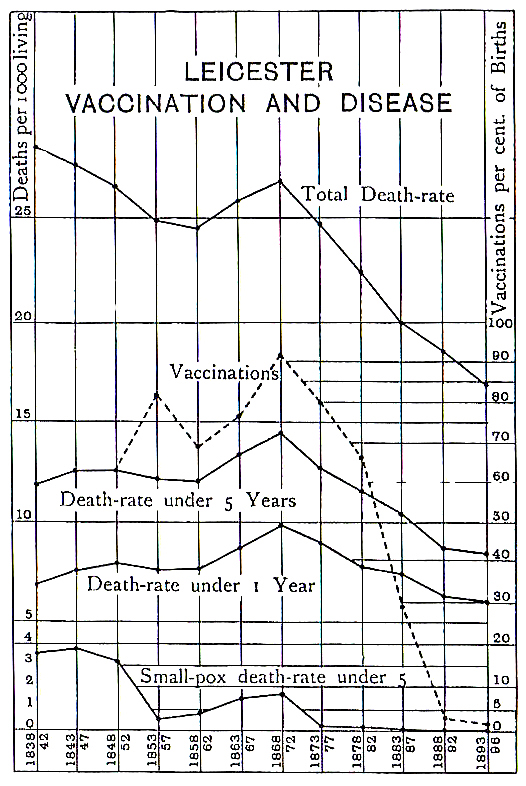
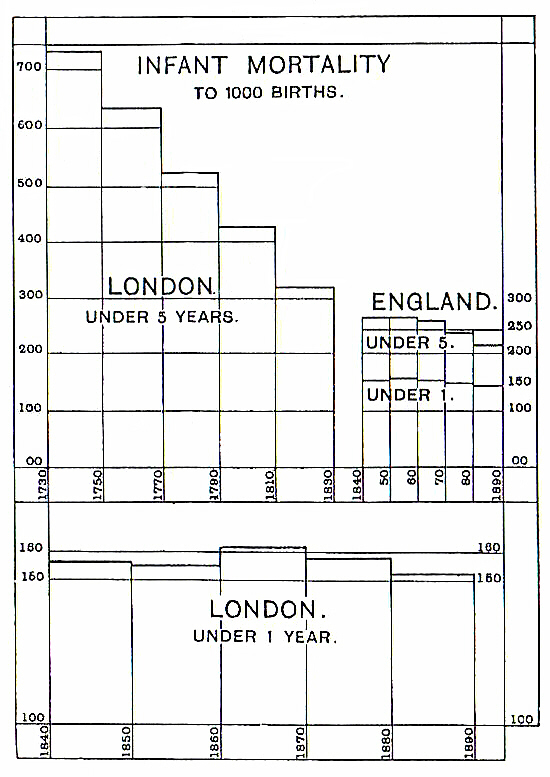
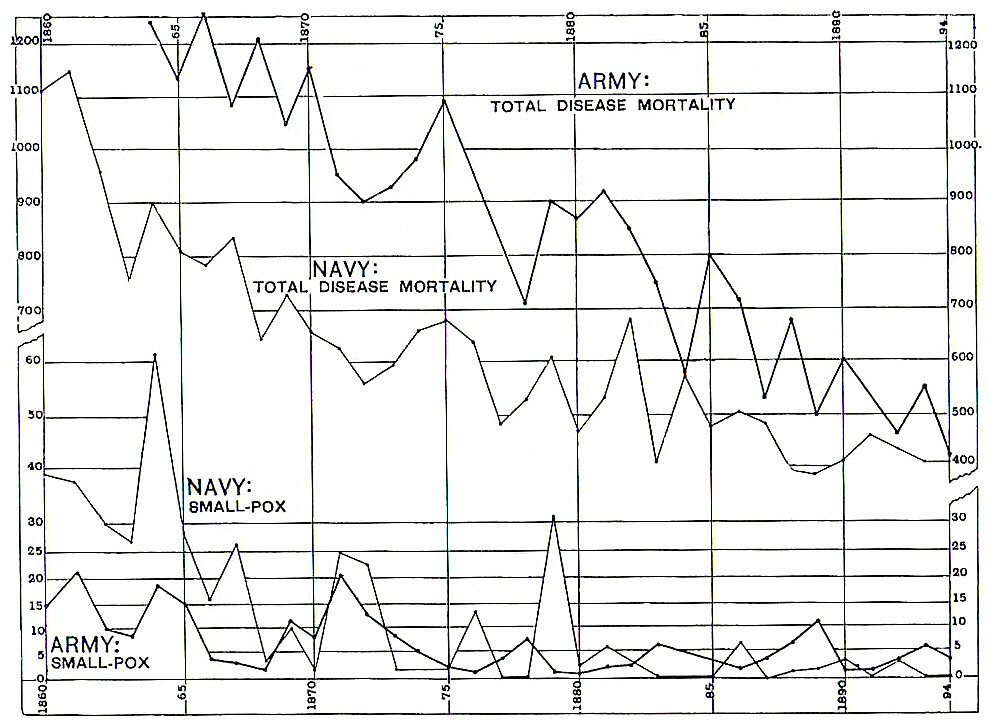
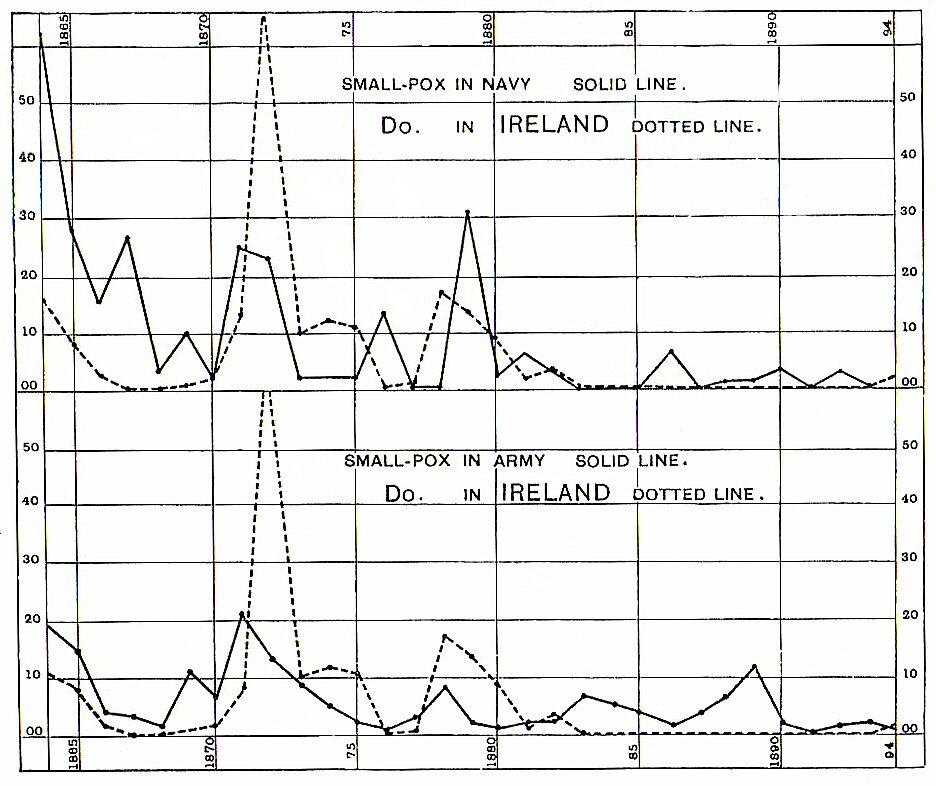






article title – DDT – Resistant Mosquitoes Spread Malaria.
Controversial insecticide is still used in the THIRD WORLD.
\”DDT was once a common insecticide in the United States, but it was banned in 1972 due to concerns & danger to wild life. It\’s still used in other countries to kill mosquitoes that spread malaria & other diseases …………. AND THAT\’S WHY THERE\’S A PROBLEM …………. WHEN MOSQUITOES BECOME RESISTANT TO DDT.\”
How could it be true ?
How could it be possible that a tiny insect like a mosquito can develop a resistance to a deadly toxin like DDT ?
It is the female mosquito that carries the malaria.
The female mosquito lives for month – in that time she lays eggs & then she dies.
How can such a tiny insect become resistant to a Deadly Chemical Compound like DDT ?
What we are being told is that the mosquito has MUTATED with each life cycle – INTO A SURER SONIC INSECT.
ONLY A SUPER SONIC INSECT COULD BE RESISTANT DDT.
New Scientist – article title – DDT finally linked to human health problems by Emma Young – 13 July 2001.
Why are we still spraying DDT in the majority of the world as a combatant to malaria carrying mosquitoes ?
Is the population / are the people of Africa more resilient & therefore they will not be affected by the toxicity that DDT is ?
Is it become the populations of Africa are poor that we spray such a dangerous toxin all over them & their food & water – over their environment.
Well then – if we do not care about the people / the human beings – Surely -then we should care about the wild life & the plant life enough to stop spraying DDT all over it.
Never will I believe that mosquitoes are resistant to DDT – it is a blatant lie.
Questo stupido robot sta accendendo i miei nervi – che cosa faccio qui nella prima parte – che ho posto per essere.
There are VAST Poppy Fields in – Nigeria – Afghanistan – Pakistan that feed the illegal global opoid trade.
Polio is still affecting the populations of – Nigeria – Afghanistan – Pakistan.
Is it possible that the VAST Poppy Fields in – Nigeria – Afghanistan – Pakistan are being sprayed with DDT ?
DDT which is then ingested by illegal drug users all around the world.